by: Baydurin S.A.
Prepared by: Issabayeva A.
463 GM
Astana, 2018
- Главная
- Разное
- Дизайн
- Бизнес и предпринимательство
- Аналитика
- Образование
- Развлечения
- Красота и здоровье
- Финансы
- Государство
- Путешествия
- Спорт
- Недвижимость
- Армия
- Графика
- Культурология
- Еда и кулинария
- Лингвистика
- Английский язык
- Астрономия
- Алгебра
- Биология
- География
- Детские презентации
- Информатика
- История
- Литература
- Маркетинг
- Математика
- Медицина
- Менеджмент
- Музыка
- МХК
- Немецкий язык
- ОБЖ
- Обществознание
- Окружающий мир
- Педагогика
- Русский язык
- Технология
- Физика
- Философия
- Химия
- Шаблоны, картинки для презентаций
- Экология
- Экономика
- Юриспруденция
acute and chronic pyelonephritis [Восстановленный] презентация
Содержание
- 1. acute and chronic pyelonephritis [Восстановленный]
- 2. Pyelonephritis is a bacterial infection of the
- 3. Incidence: About 3 to 7 out of
- 4. Grading of VUR
- 5. Causative organisms: Gram negative organism: E.coli
- 6. Pathogenesis The urinary tract can be viewed
- 8. Signs and symptoms Signs and symptoms of
- 9. Acute pyelonephritis Acute pyelonephritis is an exudative
- 10. Chronic pyelonephritis Chronic pyelonephritis implies recurrent kidney
- 12. Tubulointerstitial nephritis caused by drugs Drugs may
- 13. Acute drug induced tubulointerstitial nephritis may be
- 14. Diagnostics Physical examination: - soreness in palpation
- 15. Imaging studies If a kidney stone is
- 16. Purpose of treatment: consists in elimination of
- 17. Detoxification therapy: plentiful drink; parenteral infusion therapy
- 18. The list of basic medicines: 1. Amoxicillin
- 19. Complications If left untreated, a kidney infection
Слайд 1JSC “Astana Medical University”
Department of Internal Diseases №1
IWS
Acute and Chronic pyelonephritis
Checked

Слайд 2Pyelonephritis is a bacterial infection of the kidneys.
Pyelonephritis can be
acute or chronic, and it is most often due to the ascent of bacteria from the bladder up the ureters to infect the kidneys; it is usually bilateral. Disease affects the women more than men.

Слайд 3Incidence:
About 3 to 7 out of 10,000 people.
Predisposing factors:
Obstruction of the
urinary tract with stasis of urine
Female: Shorter urethra
Male : uncircumcised infant bacterial colonization inside prepuce and urethra
Vesicoureteric reflux: Normally, the urine does not ascend along the ureters during micturition due to the oblique course of the intravesical portion of the ureter, which provide asphincter-like effect during contraction of the bladder.) If this effect is disturbed due to congenital or acquired reasons, the urine will ascend along the ureter and may even reach the kidneys during bladder emptying.
Bilharsisis
Instrumentation of the urinary tract.
Diabetes mellitus
Female more due to short urethra.
Pregnancy due to hormonal relaxation of smooth muscle and pressure of the gravid uterus
Female: Shorter urethra
Male : uncircumcised infant bacterial colonization inside prepuce and urethra
Vesicoureteric reflux: Normally, the urine does not ascend along the ureters during micturition due to the oblique course of the intravesical portion of the ureter, which provide asphincter-like effect during contraction of the bladder.) If this effect is disturbed due to congenital or acquired reasons, the urine will ascend along the ureter and may even reach the kidneys during bladder emptying.
Bilharsisis
Instrumentation of the urinary tract.
Diabetes mellitus
Female more due to short urethra.
Pregnancy due to hormonal relaxation of smooth muscle and pressure of the gravid uterus


Слайд 5Causative organisms:
Gram negative organism: E.coli (common), Proteus mirabilis, Citrobacter, klebsiella,
enterobacter, proteus pseudomonas aeruginosa;
Gram positive organism, Staph.saprophyticus, Staph.epidermidis enterococcus, Corynebacteria and lactobacilli.
Routes of infection:
Ascending infection from the lower urinary tract.
Lymphatic spread from the intestinal tract.
Blood borne infection complicating boils or carbuncles.
Pathology:
Acute pyelonephritis
Chronic pyelonephritis
Gram positive organism, Staph.saprophyticus, Staph.epidermidis enterococcus, Corynebacteria and lactobacilli.
Routes of infection:
Ascending infection from the lower urinary tract.
Lymphatic spread from the intestinal tract.
Blood borne infection complicating boils or carbuncles.
Pathology:
Acute pyelonephritis
Chronic pyelonephritis
, Proteus mirabilis, Citrobacter, klebsiella, enterobacter, proteus pseudomonas aeruginosa;Gram")
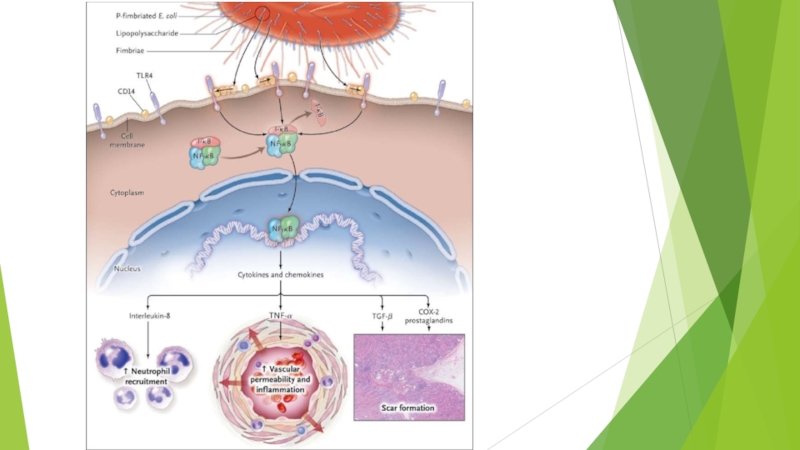
Слайд 6Pathogenesis
The urinary tract can be viewed as an anatomic unit united
by a continuous column of urine extending from the urethra to the kidneys. In the majority of UTIs bacteria establish infection by ascending from the urethra to the bladder. Continuing ascent up the ureter to the kidney is the pathway for most renal parenchymal infections.

Слайд 8Signs and symptoms
Signs and symptoms of a kidney infection might include:
Fever
Chills
Back,
side (flank) or groin pain
Abdominal pain
Frequent urination
Strong, persistent urge to urinate
Burning sensation or pain when urinating
Nausea and vomiting
Pus or blood in your urine (hematuria)
Urine that smells bad or is cloudy
Abdominal pain
Frequent urination
Strong, persistent urge to urinate
Burning sensation or pain when urinating
Nausea and vomiting
Pus or blood in your urine (hematuria)
Urine that smells bad or is cloudy
 or groin")
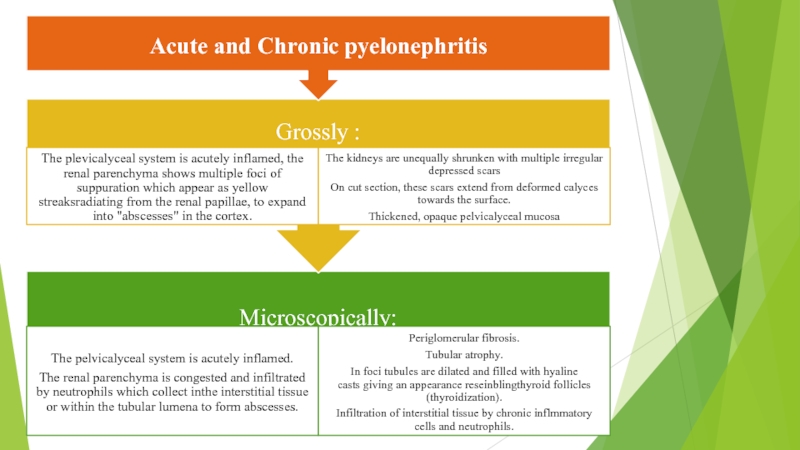
Слайд 9Acute pyelonephritis
Acute pyelonephritis is an exudative purulent localized inflammation of the renal
pelvis (collecting system) and kidney.
The kidney parenchyma presents in the interstitium abscesses (suppurative necrosis), consisting in purulent exudate (pus): neutrophils, fibrin, cell debris and central germ colonies (hematoxylinophils). Tubules are damaged by exudate and may contain neutrophil casts. In the early stages, the glomerulus and vessels are normal. Gross pathology often reveals pathognomonic radiations of bleeding and suppuration through the renal pelvis to the renal cortex.
The kidney parenchyma presents in the interstitium abscesses (suppurative necrosis), consisting in purulent exudate (pus): neutrophils, fibrin, cell debris and central germ colonies (hematoxylinophils). Tubules are damaged by exudate and may contain neutrophil casts. In the early stages, the glomerulus and vessels are normal. Gross pathology often reveals pathognomonic radiations of bleeding and suppuration through the renal pelvis to the renal cortex.
 and kidney.The kidney")
Слайд 10Chronic pyelonephritis
Chronic pyelonephritis implies recurrent kidney infections and can result in scarring of
the renal parenchyma and impaired function, especially in the setting of obstruction. A perinephric abscess (infection around the kidney) and/or pyonephrosis may develop in severe cases of pyelonephritis.
Chronic pyelonephritis with reduced kidney size and focal cortical thinning. Measurement of kidney length on the US image is illustrated by ‘+’ and a dashed line.

Слайд 12Tubulointerstitial nephritis caused by drugs
Drugs may produce renal injury by three
mechanisms:
An immunologic (allergic, hypersensitivity) reaction leading to an acute interstitial nephritis.
Direct nephrotoxicity leading to acute tubular necrosis.
Slowly progressive damage to the tubules leading to a chronic tubulointerstitial nephritis.
An immunologic (allergic, hypersensitivity) reaction leading to an acute interstitial nephritis.
Direct nephrotoxicity leading to acute tubular necrosis.
Slowly progressive damage to the tubules leading to a chronic tubulointerstitial nephritis.
")
Слайд 13Acute drug induced tubulointerstitial nephritis may be induced by synthetic penicillins
(methicillin, ampicillin), sulfonamides, rifampin, diuretics (thiazides) and non steroidal antin-flammatory drugs (phenyl butazone). It is characterized clinically by acute renal insufficiency that typically starts two weeks after the beginning of drug administration.
Acute tubular necrosis, due to direct nephrotoxicity may be induced by antibiotics (gentamicin) and antifungal agents (amphotericin B). It leads to acute renal failure.
Chronic tubulointerstitial nephritis may be induced by heavy usage of analgesic, mainly those containing phenacetin (analgesic nephropathy). It may end in chronic renal failure.
Acute tubular necrosis, due to direct nephrotoxicity may be induced by antibiotics (gentamicin) and antifungal agents (amphotericin B). It leads to acute renal failure.
Chronic tubulointerstitial nephritis may be induced by heavy usage of analgesic, mainly those containing phenacetin (analgesic nephropathy). It may end in chronic renal failure.
, sulfonamides, rifampin,")
Слайд 14Diagnostics
Physical examination:
- soreness in palpation in the area of the projection
of the kidneys;
- arterial hypertension.
Laboratory research:
- bacteriuria 105;
- leukocyturia;
- erythrocyturia;
- proteinuria (β2-microglobulin);
- reduction of the concentration function;
- GFR;
- anemia
- arterial hypertension.
Laboratory research:
- bacteriuria 105;
- leukocyturia;
- erythrocyturia;
- proteinuria (β2-microglobulin);
- reduction of the concentration function;
- GFR;
- anemia

Слайд 15Imaging studies
If a kidney stone is suspected (e.g. on the basis
of characteristic colicky pain or the presence of a disproportionate amount of blood in the urine), a kidneys, ureters, and bladder x-ray may assist in identifying radioopaque stones. Where available, a noncontrast helical CT scan with 5 millimeter sections is the diagnostic modality of choice in the radiographic evaluation of suspected nephrolithiasis. All stones are detectable on CT scans except very rare stones composed of certain drug residues in the urine. In patients with recurrent ascending urinary tract infections, it may be necessary to exclude an anatomical abnormality, such as vesicoureteral reflux or polycystic kidney disease. Investigations used in this setting include kidney ultrasonography or voiding cystourethrography. CT scan or kidney ultrasonography is useful in the diagnosis of xanthogranulomatous pyelonephritis; serial imaging may be useful for differentiating this condition from kidney cancer.
Ultrasound findings that indicate pyelonephritis are enlargement of the kidney, edema in the renal sinus or parenchyma, bleeding, loss of corticomedullary differentiation, abscess formation, or an areas of poor blood flow on doppler ultrasound. However, ultrasound findings are seen in only 20% to 24% of people with pyelonephritis.
A DMSA scan is a radionuclide scan that uses dimercaptosuccinic acid in assessing the kidney morphology. It is now the most reliable test for the diagnosis of acute pyelonephritis.
Ultrasound findings that indicate pyelonephritis are enlargement of the kidney, edema in the renal sinus or parenchyma, bleeding, loss of corticomedullary differentiation, abscess formation, or an areas of poor blood flow on doppler ultrasound. However, ultrasound findings are seen in only 20% to 24% of people with pyelonephritis.
A DMSA scan is a radionuclide scan that uses dimercaptosuccinic acid in assessing the kidney morphology. It is now the most reliable test for the diagnosis of acute pyelonephritis.

Слайд 16Purpose of treatment: consists in elimination of infectious and inflammatory process,
possible only at restoration of outflow of urine and sanitation of urinary tract.
Indications for hospitalization: In acute secondary pyelonephritis, urgent hospitalization is necessary in the urological department in connection with the possible need for an urgent open surgery to prevent severe, life-threatening complications (toxic shock). In acute primary pyelonephritis, hospitalization is also desirable, since a concealed violation is possible outflow of urine. In addition, with this form of the disease, the serous phase can quickly progress to purulent, requiring urgent surgical treatment. In extreme cases, with confidence in the diagnosis of acute primary pyelonephritis, antibiotic therapy can also be started on an outpatient basis.
Unambiguously patients need the emergency hospitalization:
▪ with acute pyelonephritis of a single or only functioning kidney;
▪ exacerbation of chronic pyelonephritis and signs of renal insufficiency;
▪ acute pyelonephritis on the background of diabetes mellitus or immunodeficiency;
▪ suspected purulent process in the kidney;
▪ acute pyelonephritis with ineffective antibiotic therapy.
Indications for hospitalization: In acute secondary pyelonephritis, urgent hospitalization is necessary in the urological department in connection with the possible need for an urgent open surgery to prevent severe, life-threatening complications (toxic shock). In acute primary pyelonephritis, hospitalization is also desirable, since a concealed violation is possible outflow of urine. In addition, with this form of the disease, the serous phase can quickly progress to purulent, requiring urgent surgical treatment. In extreme cases, with confidence in the diagnosis of acute primary pyelonephritis, antibiotic therapy can also be started on an outpatient basis.
Unambiguously patients need the emergency hospitalization:
▪ with acute pyelonephritis of a single or only functioning kidney;
▪ exacerbation of chronic pyelonephritis and signs of renal insufficiency;
▪ acute pyelonephritis on the background of diabetes mellitus or immunodeficiency;
▪ suspected purulent process in the kidney;
▪ acute pyelonephritis with ineffective antibiotic therapy.

Слайд 17Detoxification therapy:
plentiful drink;
parenteral infusion therapy in the form of solutions of
glucose 5-10% and NaCl 0.45% is indicated only for dyspepsia (nausea, vomiting, diarrhea).
Antibiotic therapy: The basic principle is the early and long-term appointment of antimicrobial agents in strict accordance with the sensitivity to them microflora inoculated from the urine, the alternation of antimicrobials or their combined use.
1. Gram-positive: semi-synthetic penicillins (ampicillin, amoxicillin + clavulanic acid).
2. Gram-negative: co-trimoxazole + fluoroquine (ciprofloxacin, ofloxacin, norfloxacin).
3. Nosocomial infection: aminoglycosides (gentamicin) + cephalosporins (ceftriaxone, cefotaxime, ceftazidime).
4. Reserve antibiotics: imipenem, amikacin.
5. Uroantiseptics: nitrofurans (furagin).
The duration of antibiotic therapy is determined by the severity of the infection process, the presence of complications.
In some cases, supportive therapy with other antibacterial agents - uroseptics (furagin 1-2 mg / kg / night, co-trimoxazole - 120-240 mg per night) is necessary.
In parallel, it is necessary to carry out antifungal therapy (itraconazole), correction of intestinal microflora, immunostimulant therapy.
Antibiotic therapy: The basic principle is the early and long-term appointment of antimicrobial agents in strict accordance with the sensitivity to them microflora inoculated from the urine, the alternation of antimicrobials or their combined use.
1. Gram-positive: semi-synthetic penicillins (ampicillin, amoxicillin + clavulanic acid).
2. Gram-negative: co-trimoxazole + fluoroquine (ciprofloxacin, ofloxacin, norfloxacin).
3. Nosocomial infection: aminoglycosides (gentamicin) + cephalosporins (ceftriaxone, cefotaxime, ceftazidime).
4. Reserve antibiotics: imipenem, amikacin.
5. Uroantiseptics: nitrofurans (furagin).
The duration of antibiotic therapy is determined by the severity of the infection process, the presence of complications.
In some cases, supportive therapy with other antibacterial agents - uroseptics (furagin 1-2 mg / kg / night, co-trimoxazole - 120-240 mg per night) is necessary.
In parallel, it is necessary to carry out antifungal therapy (itraconazole), correction of intestinal microflora, immunostimulant therapy.

Слайд 18The list of basic medicines:
1. Amoxicillin + clavulanic acid, coated tablets
250 mg / 125 mg, 500 mg / 125 mg, 875 mg / 125 mg, powder for the preparation of a solution for intravenous administration in vials 500 mg / 100 mg
2. Ampicillin - 500 mg, fl.
3. Ceftriaxone 500 mg, 1 g, fl.
4. Imipenems
5. Fluoroquine (ciprofloxacin, ofloxacin, norfloxacin)
6. Co-trimoxazole - 120 mg, 480 mg, tab.
7. Cefuroxime axetil - 125 mg, 250 mg, tablets, suspensions
8. Gentamicin 40 mg, 80 mg, fl.
9. Furagin 50 mg, tab.
10. Enalapril 5 mg, 10 mg, tab.
2. Ampicillin - 500 mg, fl.
3. Ceftriaxone 500 mg, 1 g, fl.
4. Imipenems
5. Fluoroquine (ciprofloxacin, ofloxacin, norfloxacin)
6. Co-trimoxazole - 120 mg, 480 mg, tab.
7. Cefuroxime axetil - 125 mg, 250 mg, tablets, suspensions
8. Gentamicin 40 mg, 80 mg, fl.
9. Furagin 50 mg, tab.
10. Enalapril 5 mg, 10 mg, tab.

Слайд 19Complications
If left untreated, a kidney infection can lead to potentially serious
complications, such as:
Kidney scarring. This can lead to chronic kidney disease, high blood pressure and kidney failure.
Blood poisoning (septicemia). Your kidneys filter waste from your blood and return your filtered blood to the rest of your body. Having a kidney infection can cause the bacteria to spread through your bloodstream.
Pregnancy complications. Women who develop a kidney infection during pregnancy may have an increased risk of delivering low birth weight babies.
Kidney scarring. This can lead to chronic kidney disease, high blood pressure and kidney failure.
Blood poisoning (septicemia). Your kidneys filter waste from your blood and return your filtered blood to the rest of your body. Having a kidney infection can cause the bacteria to spread through your bloodstream.
Pregnancy complications. Women who develop a kidney infection during pregnancy may have an increased risk of delivering low birth weight babies.