- Главная
- Разное
- Дизайн
- Бизнес и предпринимательство
- Аналитика
- Образование
- Развлечения
- Красота и здоровье
- Финансы
- Государство
- Путешествия
- Спорт
- Недвижимость
- Армия
- Графика
- Культурология
- Еда и кулинария
- Лингвистика
- Английский язык
- Астрономия
- Алгебра
- Биология
- География
- Детские презентации
- Информатика
- История
- Литература
- Маркетинг
- Математика
- Медицина
- Менеджмент
- Музыка
- МХК
- Немецкий язык
- ОБЖ
- Обществознание
- Окружающий мир
- Педагогика
- Русский язык
- Технология
- Физика
- Философия
- Химия
- Шаблоны, картинки для презентаций
- Экология
- Экономика
- Юриспруденция
Podstawy chemioterapii nowotworów złośliwych презентация
Содержание
- 1. Podstawy chemioterapii nowotworów złośliwych
- 2. Cancer’s timeline
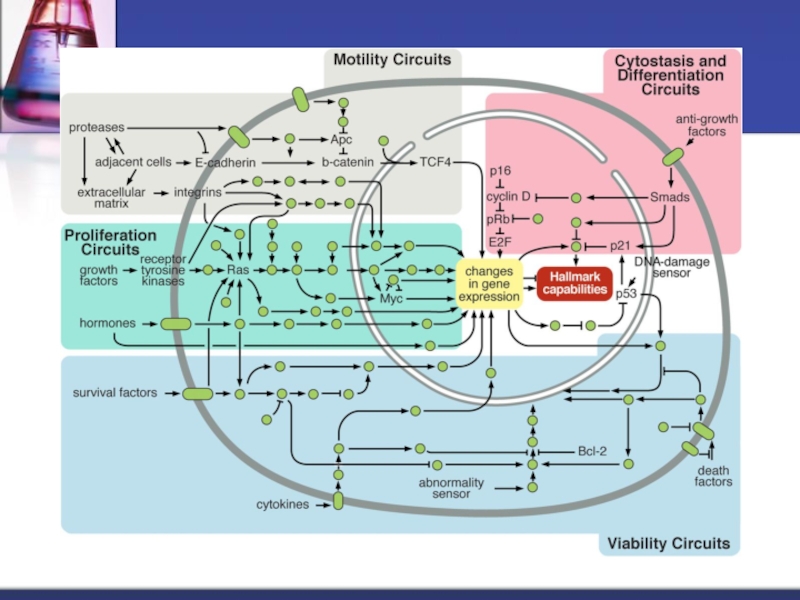
- 4. The Hallmarks of Cancer
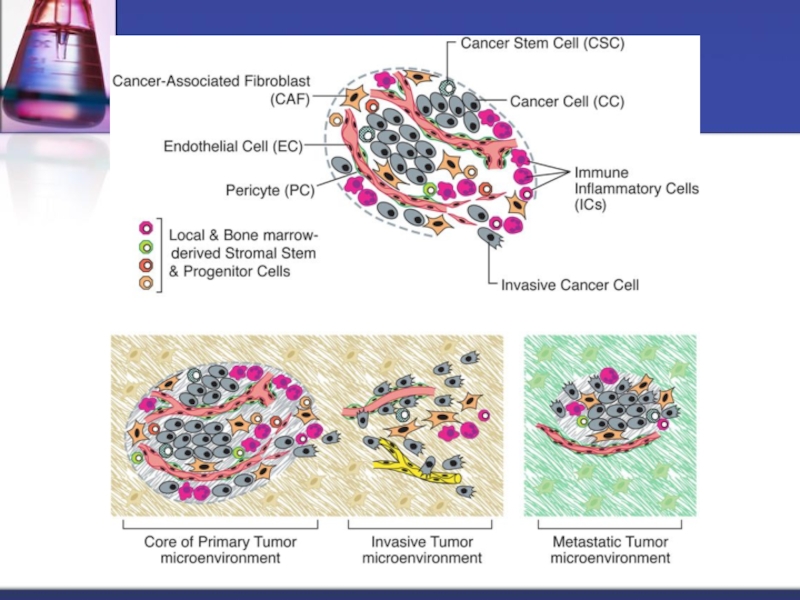
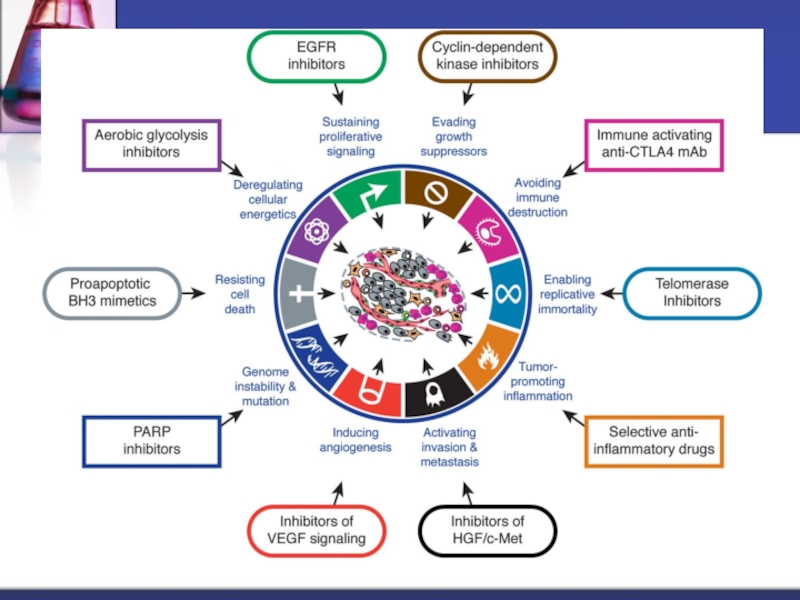
- 5. The Hallmarks of Cancer – next generation
- 8. Air raid on Bari, Italy, 2nd Dec
- 10. USS John Harvey John Harvey One of
- 12. John Singer Sargent: Gassed, 1919 Painting of
- 13. Nitrogen mustard The nitrogen mustards are cytotoxic
- 14. Mustine (metchloramine)
- 15. Chlormethine (INN (INN, BAN), mechlorethamine (widely
- 16. Key advances in the history of cancer
- 17. Key advances in the history of cancer
- 18. The current position of chemotherapy for advanced
- 19. At the other end of the
- 20. In the middle, we have a
- 21. High-cost drugs can achieve extension of
- 22. Currently, most cytotoxic agents exert their effect
- 23. Cykl komórkowy Leczenie chemiczne jest ściśle powiązane z fizjologią komórki
- 24. Badania Skippera i Schabela 1. Określona dawka
- 26. KRZYWA GOMPERTZA Okres początkowy Mała ilość
- 27. KRZYWA GOMPERTZA (oporność na leczenie) Okres
- 28. Grupy leków przeciwnowotworowych Leki alkilujące Antymetabolity Kwasu
- 29. Podział cytostatyków ze względu na mechanizm działania
- 30. Leki alkilujące (niezależne od fazy) Przyłączanie rodników
- 31. Cyclophosphamide (CTX) Activated by the liver cytochrome
- 32. Ifosfamide Activated by the liver cytochrome P450
- 33. Cisplatin Platinum analog, covalently binds to DNA
- 34. Antymetabolity (zależne od fazy – S) Strukturalne
- 35. 5-Fluorouracil Antimetabolite, fluoropirymidine analog Requires activation to
- 36. Inhibitory topoizomerazy I (niezależne od fazy) Topoaktywne
- 37. Irinotecan Topoisomerase I inhibitor, semisynthetic derivative of
- 38. Antybiotyki cytotoksyczne (swoiste fazowo – S) Wieloraki
- 39. Doxorubicin Antitumor antibiotic isolated from Streptomyces species
- 40. Alkaloidy (swoiste fazowo – M) Wiążą
- 41. Vincristine Antimicrotubule agent, vinca alkaloid derived from
- 42. Taksoidy (swoiste fazowo – M) Hamują
- 43. Docetaxel Antimicrotubule, semisynthetic agent, derived from the
- 44. Lignany (swoiste fazowo – G2, M)
- 45. Etoposide Topoisomerase II inhibitor, plant alkaloid extracted
- 46. Podział chemioterapii ze względu na stosunek
- 47. Podział chemioterapii ze względu na drogę
- 48. Podstawowe zasady chemioterapii nowotworów 1. Leczenie choroby
- 49. Podstawowe zasady chemioterapii nowotworów 4. Konieczne jest
- 50. Podstawowe zasady chemioterapii nowotworów c. stosowane preparaty
- 51. Podstawowe zasady chemioterapii nowotworów 6. Niszczenie masy
- 52. Podstawowe zasady chemioterapii nowotworów 7. Niezbędnym elementem
- 53. Monitorowanie leczenia Skala wydolności chorego ECOG/WHO Skala
- 54. Skala wydolności chorego ECOG/WHO
- 55. Kryteria odpowiedzi na leczenie RECIST CR (Całkowita
- 56. Definicja wyleczenia Russela „O wyleczeniu chorego z
- 57. Wreszcie koniec
Слайд 1Podstawy chemioterapii nowotworów złośliwych
Klinika Onkologii Uniwersytet Medyczny w Białymstoku




Слайд 8Air raid on Bari, Italy, 2nd Dec 1943
The air raid on
The attack, which lasted a little more than one hour, put the port out of action until February 1944 and was called the "Little Pearl HarborThe attack, which lasted a little more than one hour, put the port out of action until February 1944 and was called the "Little Pearl Harbor". The release of mustard gas from one of the wrecked cargo ships added to the loss of life. The British and US governments covered up the presence of mustard gas and its effects on victims of the raid.


Слайд 10USS John Harvey
John Harvey
One of the destroyed vessels—the U.S. Liberty ship
Within a day, the first symptoms of mustard poisoning had appeared in 628 patients and medical staff, with symptoms including blindness and chemical burns. This puzzling development was further complicated by the arrival of hundreds of Italian civilians also seeking treatment, who had been poisoned by a cloud of sulfur mustard vapor that had blown over the city when some of the John Harvey's cargo exploded. As the medical crisis worsened, little information was available about what was causing these symptoms, as the U.S. military command wanted to keep the presence of chemical munitions secret from the Germans.[29] Nearly all crewmen of the John Harvey had been killed, and were unavailable to explain the cause of the "garlic-like" odor noted by rescue personnel.[27]
Informed about the mysterious symptoms, Deputy Surgeon General Fred Blesse sent for Lieutenant Colonel Stewart Francis Alexander, an expert in chemical warfare. Carefully tallying the locations of the victims at the time of the attack, Alexander traced the epicenter to the John Harvey, and confirmed mustard gas as the responsible agent when he located a fragment of the casing of a U.S. M47A1 bomb.[3]
By the end of the month, 83 of the 628 hospitalized military victims had died. The number of civilian casualties, thought to have been even greater, could not be accurately gauged since most had left the city to seek shelter with relatives.[3]
The U.S. destroyer escortThe U.S. destroyer escort (DE)—USS Bistera—though lightly damaged—picked up survivors from the water during the raid and put out to sea; during the night members of the crew went blind and developed chemical burns. The Bistera had to return, with great difficulty, to Taranto harbour.[30][30][31]
Cover-up
A member of Allied Supreme Commander General Dwight D. EisenhowerA member of Allied Supreme Commander General Dwight D. Eisenhower's medical staff, Dr. Stewart F. Alexander, was dispatched to Bari following the raid. Alexander had trained at the Army's Edgewood Arsenal in Maryland, and was familiar with some of the effects of mustard gas. Although he was not informed of the cargo carried by the SS John Harvey, and most victims suffered atypical symptoms caused by exposure to mustard diluted in water and oil (as opposed to airborne), Alexander rapidly concluded that mustard gas was present. Although he could not get any acknowledgment from the chain of command, Alexander convinced medical staffs to treat patients for mustard gas exposure and saved many lives as a result. He also preserved many tissue samples from autopsied victims at Bari. After WWII, these samples would result in the development of an early form of chemotherapy, and most victims suffered atypical symptoms caused by exposure to mustard diluted in water and oil (as opposed to airborne), Alexander rapidly concluded that mustard gas was present. Although he could not get any acknowledgment from the chain of command, Alexander convinced medical staffs to treat patients for mustard gas exposure and saved many lives as a result. He also preserved many tissue samples from autopsied victims at Bari. After WWII, these samples would result in the development of an early form of chemotherapy based on mustard, Mustine.[32]
From the start, Allied High Command tried to conceal the disaster, in case the Germans believed that the Allies were preparing to use chemical weapons, which might provoke them into preemptive use, but there were too many witnesses to keep the secret, and in February 1944, the U.S. Chiefs of Staff issued a statement admitting to the accident and emphasizing that the U.S. had no intention of using chemical weapons except in the case of retaliation.[31]
General Dwight D. Eisenhower approved Dr. Alexander's report. Winston Churchill, however, ordered all British documents to be purged, listing mustard gas deaths as "burns due to enemy action".[3]
U.S. records of the attack were declassified in 1959, but the episode remained obscure until 1967 when author Glenn B. Infield published the book Disaster at Bari.[32] In 1986 the British government finally admitted to survivors of the Bari raid that they had been exposed to poison gas and amended their pension payments accordingly.[33]
In his autobiographical work Destroyer Captain published in 1975 by William Kimber & Co, Lieutenant Commander Roger Hill describes refuelling HMS Grenville in Bari shortly after the attack. He describes the damage done and details how a shipload of mustard gas came to be in the harbour because of intelligence reports which he viewed as "incredible".
In 1988, through the efforts of Nick T. SparkIn 1988, through the efforts of Nick T. Spark, U.S. Senator Dennis DeConciniIn 1988, through the efforts of Nick T. Spark, U.S. Senator Dennis DeConcini and U.S. Senator Bill BradleyIn 1988, through the efforts of Nick T. Spark, U.S. Senator Dennis DeConcini and U.S. Senator Bill Bradley, Alexander received recognition from the Surgeon General of the United States Army for his actions in the aftermath of the Bari disaster.[34]
Aftermath
A subsequent inquiry exonerated Coningham but found that the absence of previous air attacks had led to complacency.[6]

Слайд 12John Singer Sargent: Gassed, 1919 Painting of a line of soldiers walking

Слайд 13Nitrogen mustard
The nitrogen mustards are cytotoxic are cytotoxic chemotherapy are cytotoxic
During WWII nitrogen mustards were studied at the Yale School of MedicineDuring WWII nitrogen mustards were studied at the Yale School of Medicine by Alfred GilmanDuring WWII nitrogen mustards were studied at the Yale School of Medicine by Alfred Gilman and Louis Goodman, and classified human clinical trials of nitrogen mustards for the treatment of lymphoma started in December 1942.[9] Also during WWII, an incident during the air raid on Bari, Italy, led to the release of mustard gas that affected several hundred soldiers and civilians.[10] Medical examination of the survivors showed a decreased number of lymphocytes.[11] After WWII was over, the Bari incident and the Yale group's studies eventually converged prompting a search for other similar compounds. Due to its use in previous studies, the nitrogen mustard known as "HN2" became the first chemotherapy known as "HN2" became the first chemotherapy drug mustine.
Nitrogen mustards are not related to the mustard plantNitrogen mustards are not related to the mustard plant or its pungent essence, allyl isothiocyanate: the name comes from the pungent smell of chemical weapons preparations.

")
Слайд 15
Chlormethine (INN (INN, BAN), mechlorethamine (widely used in the US, not
Successful clinical use of chlormethine (mechlorethamine) resulted in development of the field of anticancer chemotherapy, led by Cornelius P. RhoadsSuccessful clinical use of chlormethine (mechlorethamine) resulted in development of the field of anticancer chemotherapy, led by Cornelius P. Rhoads at Memorial Sloan-KetteringSuccessful clinical use of chlormethine (mechlorethamine) resulted in development of the field of anticancer chemotherapy, led by Cornelius P. Rhoads at Memorial Sloan-Kettering. The drug is a nitrogen-based analogue of mustard gasSuccessful clinical use of chlormethine (mechlorethamine) resulted in development of the field of anticancer chemotherapy, led by Cornelius P. Rhoads at Memorial Sloan-Kettering. The drug is a nitrogen-based analogue of mustard gas (which is sulfur-based) and was derived from chemical warfareSuccessful clinical use of chlormethine (mechlorethamine) resulted in development of the field of anticancer chemotherapy, led by Cornelius P. Rhoads at Memorial Sloan-Kettering. The drug is a nitrogen-based analogue of mustard gas (which is sulfur-based) and was derived from chemical warfare research. Secret clinical trials of the agent for Hodgkin's diseaseSuccessful clinical use of chlormethine (mechlorethamine) resulted in development of the field of anticancer chemotherapy, led by Cornelius P. Rhoads at Memorial Sloan-Kettering. The drug is a nitrogen-based analogue of mustard gas (which is sulfur-based) and was derived from chemical warfare research. Secret clinical trials of the agent for Hodgkin's disease and several other lymphomasSuccessful clinical use of chlormethine (mechlorethamine) resulted in development of the field of anticancer chemotherapy, led by Cornelius P. Rhoads at Memorial Sloan-Kettering. The drug is a nitrogen-based analogue of mustard gas (which is sulfur-based) and was derived from chemical warfare research. Secret clinical trials of the agent for Hodgkin's disease and several other lymphomas and leukemias in humans began in December 1942. Because of wartime secrecy restrictions, it was not until 1946 that the results of these trials were published openly.[14]
, mechlorethamine (widely used in the US, not the USAN, however) also")
Слайд 16Key advances in the history of cancer chemotherapy.
DeVita V T ,
©2008 by American Association for Cancer Research

Слайд 17Key advances in the history of cancer chemotherapy.
DeVita V T ,
©2008 by American Association for Cancer Research

Слайд 18The current position of chemotherapy for advanced cancer
Essentially, there are
This first group includes diseases such as Hodgkin’s disease, childhood leukaemia and testicular cancer (less than 5% of the global cancer burden)

Слайд 19
At the other end of the spectrum, we have a group

Слайд 20
In the middle, we have a group of diseases with a

Слайд 21
High-cost drugs can achieve extension of life by several months for

Слайд 22Currently, most cytotoxic agents exert their effect by interfering with the


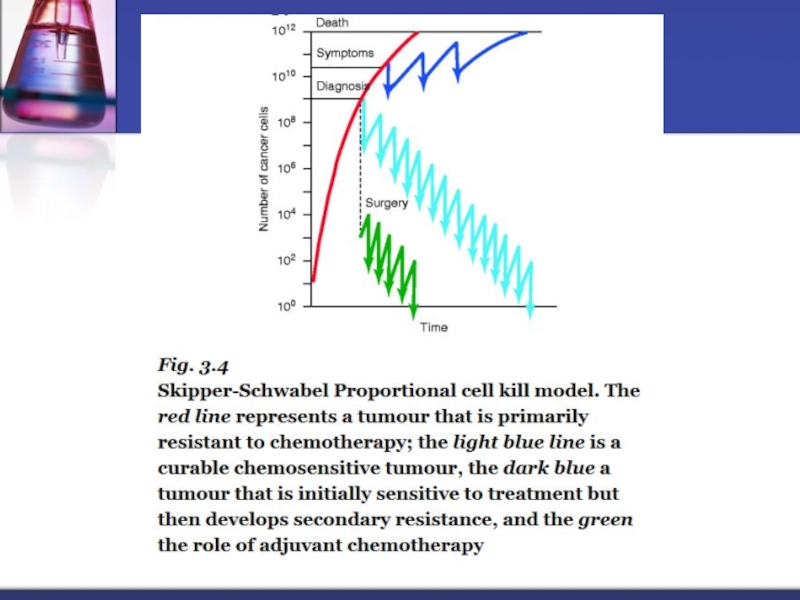
Слайд 24Badania Skippera i Schabela
1. Określona dawka leku cytostatycznego niszczy zawsze ten
2. Chemioterapeutyki wywierają efekt cytotoksyczny niemal wyłącznie w stosunku do komórek dzielących się (frakcja komórek proliferujących).

Слайд 26KRZYWA GOMPERTZA
Okres początkowy
Mała ilość komórek nowotworowych
bardzo dużo komórek proliferujących
krótki czas podwajania
Choroba w zaawansowanym stadium Duża ilość komórek nowotworowych mało komórek proliferujących dużo komórek w fazie spoczynkowej G0 długi czas podwajania masy guza
angiogeneza
Opisuje wzrost nowotworów litych, w funkcji czasu i ilości komórek nowotworowych

Слайд 27KRZYWA GOMPERTZA
(oporność na leczenie)
Okres początkowy
Mała częstość mutacji
komórki nowotoworowe wrażliwe na stosowane
Choroba w zaawansowanym stadium Duża częstość mutacji Dużo komórek opornych na leczenie
Okres początkowy Mała częstość mutacji komórki nowotoworowe wrażliwe na stosowane leczenieChoroba")
Слайд 28Grupy leków przeciwnowotworowych
Leki alkilujące
Antymetabolity
Kwasu foliowego
Pirymidyn
Puryn
Inhibitory deaminazy adenozynowej
Inne antymetabolity
Inhibitory topoizomerazy
Antybiotyki cytostatyczne
Alkaloidy
Taksoidy
Lignany
Enzymy
Hormony
Inne leki

Слайд 29Podział cytostatyków ze względu na mechanizm działania
Fazozależne
Podanie tej samej dawki sytostatyku
Ich działanie jest tym skuteczniejsze im więcej komórek proliferujących znajduje się w populacji.
Fazoniezależne
Wynik ich działania jest
Wprost proporcjonalny do
wielkości dawki jednorazowej.
Działają w tych nowotworach, w których odsetek komórek proliferujących jest niewielki

Слайд 30Leki alkilujące
(niezależne od fazy)
Przyłączanie rodników alkilowych do grup funkcyjnych cząsteczek o
Alkilacja powoduje rozluźnienie wiązania zasady azotowej z resztą cukrową, depurynację, rozpad łańcucha głównego DNA.
CYKLIFOSFAMID
IFOSFAMID
MELFALAN
BUSULFAN
STREPTOZOCYNA
DAKARBAZYNA (G2)
CISPLATYNA
KARBOPLATYNA
OKSALIPLATYNA
Przyłączanie rodników alkilowych do grup funkcyjnych cząsteczek o ujemnym łądunku (np.")
Слайд 31Cyclophosphamide (CTX)
Activated by the liver cytochrome P450 to the cytotoxic metabolites
May
Require increased fluid intake, emptying bladder several times daily
Dose reduction in the setting of renal dysfuncion
Toxicity: myelotoxicity, hemorrhagic cystitis, nausea, vomiting, alopecia, amenorrea, sterility, cardiotoxicity (high dose), secondary maignancies (AML, bladder cancer), immunosupression, SIADH, hypersensitivity reactions (rhinitis, pharyngitis)
Activated by the liver cytochrome P450 to the cytotoxic metabolitesMay be given orally and")
Слайд 32Ifosfamide
Activated by the liver cytochrome P450 to various cytotoxic metabolites
Given intravenously;
Dose reduction in the setting of renal dysfuncion
Toxicity: myelotoxicity, hemorrhagic cystitis, nausea, vomiting, neurotoxicity, alopecia, amenorrea, infertility, SIADH, teratogenic

Слайд 33Cisplatin
Platinum analog, covalently binds to DNA producing cross-links (intra- or interstrand)
Dose must be reduced in the setting of renal dysfunction, vigorous hydration obligatory, potent emetogenic agent, contraindicated in patients with pre-existing hearing deficit
Toxicity: nephrotoxicity, nausea, vomiting, neurotoxicity, myelosupression, ototoxicity, hypersensitivity reactions, ocular toxicity, vascular events, including myocardial infarction, infertility, alopecia, SIADH
 ; formation of DNA")
Слайд 34Antymetabolity
(zależne od fazy – S)
Strukturalne analogi naturalnych metabolitów i koenzymów
Zahamowanie syntezy
Leczenie opiera się na różnicy kinetyki rozrostu między tkanką nowotworową, a prawidłową (szybko rosnąca tkanka pochłania większą ilość antymetabolitu)
ANTAGONIŚCI KWASU FOLIOWEGO
METOTREKSAT
EDATREKSAT
ANTAGONIŚCI PIRYMIDYN
5’-FLUOROURACYL
KAPECYTABINA
CYTARABINA
GEMCYTABINA
ANTAGONIŚCI PURYN
MERKAPTOPURYNA
AZATIPRYNA
INHIBITORY DEAMINAZY ADENOZYNOWEJ
PENTOSTATYNA
INNE ANTYMETABOLITY
FLUDARABINA
KLADRYBINA
Strukturalne analogi naturalnych metabolitów i koenzymówZahamowanie syntezy kwasów nukeinowych i")
Слайд 355-Fluorouracil
Antimetabolite, fluoropirymidine analog
Requires activation to cytotoxic metabolite forms
Inhibition of the target
Leucovorin enhances the toxicity and antitumor activity of 5-FU
Deficiency in dihydropirymidine dehydrogenase may lead to unexpected severe toxicity
Toxicity: myelosupression, diarrhoea, mucositis, hand-foot syndrome, neurotoxicity, cardiotoxicity, blepharitis, conjunctivitis, dry skin, photosensitivity, vein inflammation
;")
Слайд 36Inhibitory topoizomerazy I
(niezależne od fazy)
Topoaktywne leki stymulują i stabilizują kompleks topoizomerazy
KAPTOTECYNA
TOPOTEKAN
IRINOTEKAN
Topoaktywne leki stymulują i stabilizują kompleks topoizomerazy i DNA, powodując")
Слайд 37Irinotecan
Topoisomerase I inhibitor, semisynthetic derivative of camptothecin, an alkaloid extract from
Converted enzymatically to active metabolite SN-38 in the liver
Toxicity: myelosupression, diarrhoea, cholinergic syndrome, nausea, vomiting, alopecia, asthenia, fever

Слайд 38Antybiotyki cytotoksyczne
(swoiste fazowo – S)
Wieloraki mechanizm działania
Uszkodzenie DNA (inhibitory topoizomerazy II)
Tworzenie
Uszkadzają funkcję błony komórkowej
Antracykliny I generacji
DOKSORUBICYNA
DAUNORUBICYNA
Antracykliny II generacji
AKLARUBICYNA
EPIRUBICYNA
IDARUBICYNA
MITOKSANTRON
Inne antybiotyki cytostatyczne
DAKTYNOMYCYNA
BLEOMYCYNA (G1)
Wieloraki mechanizm działaniaUszkodzenie DNA (inhibitory topoizomerazy II)Tworzenie wolnych rodników tlenowychUszkadzają")
Слайд 39Doxorubicin
Antitumor antibiotic isolated from Streptomyces species
Mechanism of action is complex:
Intercalates into
Inhibits transcription through inhibition of DNA-dependent RNA polymerase
Inhibition of topoisomerase II leading to DNA breaks
Formation of cytotoxic oxygen free radicals leading to DNA breaks
Special considerations:
monitor cardiac function, strong vesicant, dose reduction in the setting of liver dysfunction, cumulative doses of >450mg/m2 are associated with increased risk of cardiotoxicity
Toxicity: myelosupression, nausea, vomiting, cardiotoxicity, mucositis, diarrhoea, alopecia

Слайд 40Alkaloidy
(swoiste fazowo – M)
Wiążą się z tubuliną wrzeciona kariokinetycznego, powodując
Zahamowanie podziału komórki w stadium metafazy
Chaotyczne rozmieszczenie chromosomów i śmierć komórki
WINKRYSTYNA
WINBLASTYNA
WINDEZYNA
WINORELBINA
Wiążą się z tubuliną wrzeciona kariokinetycznego, powodując jego destabilizację.Zahamowanie podziału komórki")
Слайд 41Vincristine
Antimicrotubule agent, vinca alkaloid derived from periwinkle plant Catharanthus roseus
Inhibits tubulin
Dose reduction in the setting of liver dysfunction,
Toxicity: neurotoxicity, constipation, ileus, alopecia, skin rash, fever, myelosupression, SIADH, hypersensitivity reactions, infertility

Слайд 42Taksoidy
(swoiste fazowo – M)
Hamują depolimeryzację mikrotubuli i stabilizują ją
Indukują polimeryzację
Powstają nieprawidłowe konfiguracje polimeru uniemożliwiające prawidłowe ukształtowanie się wrzeciona kariokinetycznego.
PAKLITAKSEL
DOCETAKSEL
Hamują depolimeryzację mikrotubuli i stabilizują jąIndukują polimeryzację mikrotubuliPowstają nieprawidłowe konfiguracje polimeru")
Слайд 43Docetaxel
Antimicrotubule, semisynthetic agent, derived from the needles of the European yew
High-affinity binding to microtubules enhances tubulin polymerization; normal dynamic process of microtubule network is inhibited, leading to inhibition of mitosis and cell division
Special considerations: Steroid premedication
Toxicity: Hypersensitivity reactions, myelosupression, fluid retention syndrome, skin rash, discoloration of fingernails, mucositis, diarrhoea, peripheral neuropathy, fatigue, arthralgias, myalgias

Слайд 44Lignany
(swoiste fazowo – G2, M)
Hamują przejście komórki z fazy G2
Hamują aktywność topoizomerazy II
Hamują syntezę kwasów nukleinowych
Generują wolne rodniki tlenowe
ETOPOZYD
TENIPOZYD
Hamują przejście komórki z fazy G2 do fazy MHamują aktywność")
Слайд 45Etoposide
Topoisomerase II inhibitor, plant alkaloid extracted from Podophyllum peltatum mandrake plant
Special
Toxicity: myelosupression, nausea, vomiting, anorexia, alopecia, mucositis, diarrhoea, hypersensitivity reactions, increased risk of secondary malignancies, especially AML

Слайд 46Podział chemioterapii
ze względu na stosunek do leczenia radykalnego
Chemioterapia uzupełniająca:
Neoadiuwantowa -
Adiuwantowa - polega na stosowaniu cytostatyków po leczeniu radykalnym (radioterapia, chirurgia). Postępowanie to również ma na celu zniszczenie istniejących mikroprzerzutów.
Paliatywna - stosowana jest u chorych, u których uzyskanie wyleczenia jest niemożliwe. W tym przypadku stosowanie cytostatyków ma na celu wydłużenie życia chorego i/lub poprawę jakości życia chorego.

Слайд 47Podział chemioterapii
ze względu na drogę podawania cytostatyków
Chemioterapia klasyczna (systemowa)
Chemioterapia dokanałowa
Chemioterapia
Chemioterapia lokoregionalna (dotętnicza, miejscowa, implantacja polimerów z aktywnym cytostatykiem)
Chemioterapia dokanałowaChemioterapia dojamowa (do jamy opłucnej,")
Слайд 48Podstawowe zasady chemioterapii nowotworów
1. Leczenie choroby należy zaczynać jak najwcześniej, natychmiast
2. Należy stosować największe tolerowane dawki leków z pewnymi przerwami, koniecznymi do odnowy prawidłowych tkanek organizmu.
3. Należy dążyć do maksymalnie wybiórczego zniszczenia tkanki nowotworowej z minimalnym i odwracalnym uszkodzeniem prawidłowych tkanek.

Слайд 49Podstawowe zasady chemioterapii nowotworów
4. Konieczne jest uwzględnienie wpływu leków cytostatycznych na
5. Regułą jest stosowanie terapii wielolekowej (polichemioterapii), przy uwzględnieniu następujących zasad:
a. każdy z preparatów powinien być skuteczny w monoterapii,
b. należy łączyć leki o różnym mechanizmie działania i punkcie uchwytu w cyklu komórkowym,

Слайд 50Podstawowe zasady chemioterapii nowotworów
c. stosowane preparaty powinny wykazywać synergizm działania,
d. leki
e. możliwe jest zastosowanie dawek preparatów mniejszych od stosowanych w monoterapii, dzięki temu toksyczność leczenia jest mniejsza,
f. polichemioterapia pozwala na zmniejszenie prawdopodobieństwa selekcji klonów komórek nowotworowych opornych na leczenie.

Слайд 51Podstawowe zasady chemioterapii nowotworów
6. Niszczenie masy nowotworowej jest skojarzone i etapowe,
Mobilizacja
Przyspieszenie przejścia komórek z fazy spoczynku G0 do cyklu komórkowego.
Synchronizacja
Polega na zahamowaniu jak największej liczby komórek w jednej fazie cyklu i podaniu dużej dawki leku, swoistego dla kolejnej fazy cyklu podziałowego, w celu zniszczenia jak największej ilości komórek nowotworowych.

Слайд 52Podstawowe zasady chemioterapii nowotworów
7. Niezbędnym elementem jest terapia wspomagająca i ochronna,
Fluorouracyl – w dawce 500 mg / m2 w 1 dniu terapii
Doksorubicyna – w dawce 50 mg / m2 w 1 dniu terapii
Cyklofosfamid – w dawce 500 mg / m2 w 1 dniu terapii
FAC w terapii adiuwantowej raka piersi
Cykl leczenia powtarza się co 3 tygodnie licząc od 1 dnia (co 21 dni).

Слайд 53Monitorowanie leczenia
Skala wydolności chorego ECOG/WHO
Skala toksycznosci CTC
Kryteria odpowiedzi na leczenie RECIST
(Markery nowotworowe)
")

Слайд 55Kryteria odpowiedzi na leczenie RECIST
CR (Całkowita odpowiedź)
Ustąpienie wszystkich objawów klinicznych i
PR (Częściowa odpowiedź) Zmniejszenie się o co najmniej 30% sumy największych wymiarów zmian, potwierdzone przez 2 obserwacje w odstępie co najmniej 4 tygodni. Równocześnie nie stwierdza się pojawienia nowych zmian, ani powiększenia żadnej z istniejących zmian.
SD (Stabilizacja choroby)
Zmniejszenie się o mniej niż 50% wszystkich zmian lub ich powiększenie o nie więcej niż 25% (przy uwzględnieniu w/w kryteriów).
PD (Progresja choroby)
Powiększenie się sumy największych wymiarów zmian o więcej niż 20% lub pojawienie się nowych zmian.
 Ustąpienie wszystkich objawów klinicznych i biochemicznych nowotworu, potwierdzone")
Слайд 56Definicja wyleczenia Russela
„O wyleczeniu chorego z nowotworu możemy mówić wtedy, gdy