- Главная
- Разное
- Дизайн
- Бизнес и предпринимательство
- Аналитика
- Образование
- Развлечения
- Красота и здоровье
- Финансы
- Государство
- Путешествия
- Спорт
- Недвижимость
- Армия
- Графика
- Культурология
- Еда и кулинария
- Лингвистика
- Английский язык
- Астрономия
- Алгебра
- Биология
- География
- Детские презентации
- Информатика
- История
- Литература
- Маркетинг
- Математика
- Медицина
- Менеджмент
- Музыка
- МХК
- Немецкий язык
- ОБЖ
- Обществознание
- Окружающий мир
- Педагогика
- Русский язык
- Технология
- Физика
- Философия
- Химия
- Шаблоны, картинки для презентаций
- Экология
- Экономика
- Юриспруденция
Pneumonia in children. Diagnostics and treatment презентация
Содержание
- 1. Pneumonia in children. Diagnostics and treatment
- 2. Plan of the lecture 1. Definition pneumonia
- 3. Pneumonia is a group of acute focal
- 4. Predisposed anatomy-physiologic peculiarities in children to pneumonia
- 5. Predisposing premorbid factors for pneumonia Premature
- 6. Pneumonia etiology Streptococcus Pneumonia ( 60-80% cases
- 7. All microorganisms from sputum are divided into 3 groups pathogenic provisional pathogenic nonpathogenic
- 8. Pathogenic are microorganisms with complementary receptors to
- 9. Diagnostic criteria of bacterial pneumonia Anamnestic data
- 10. Pneumonia classification in children
- 11. Focal pneumonia (30-40% of pneumonia) It frequently
- 12. Focal-confluent pneumonia Several segments are affected or
- 13. Segmental Pneumonia Pneumonia affects one or several
- 14. Interstitial pneumonia (1% of all pneumonia) Acute
- 15. Croupous pneumonia Classic example of community acquired
- 16. Respiratory Failure –is a condition of disturbed
- 17. Clinical classification of respiratory failure Grade
- 18. Main principles of pneumonia treatment Treatment must
- 19. Indications for hospitalization Infants Respiratory failure,
- 20. Pay attention for Respiratory rate (
- 21. It’s important Air humidification in room where
- 22. Etiotropic therapy Foundation of etiotropic treatment is
- 23. Main groups of antimicrobial drugs Beta-lactams 1.
- 24. Main statements of antibiotic therapy Antibiotic administration
- 25. Efficacy criteria of antibiotic therapy in pneumonia
- 26. Effects of antibiotic therapy Complete effect- temperature
- 27. Side effects of antibiotic medication
- 28. Pathogenic treatment Respiratory supplementation according to
- 29. Segmental structure of lungs (scheme)
- 30. Questions To indicate etiologic and pathophysiologic factors
- 31. Pneumonia complication- pneumothorax
- 39. Thank you

Слайд 2Plan of the lecture
1. Definition pneumonia
2. Etiology
3. Pneumonia pathogenesis
4. Classification of
pneumonia
5. Pneumonia treatment
5. Pneumonia treatment

Слайд 3Pneumonia is a group of acute focal infectious inflammatory diseases varied
in etiology, pathogenesis and morphologic characteristic with predominant involvement in pathologic process of respiratory tract with invariable presence of alveolar inflammatory exudate.

Слайд 4Predisposed anatomy-physiologic peculiarities in children to pneumonia
Trachea and big bronchi
are short and wide – easy penetration of infection
Little bronchi and bronchioli are narrow and are deficient in connective and muscular tissue – they are easily collapsed and obstructed
Inadequate drainage of several segments due to peculiarities of bronchial branching – frequent involvement of I, II, IX, X, VI segments bilateral and of IV, V segments of left lung
Lack of elastic fibers and surfactant –lung rigidity, inclination to atelectasis and emphysema development
Insufficient mucocilliar clearance – difficulties in foreign bodies removing
Insufficient synthesis of interferon and IgA – incompatibility immune response
Plethoric lung parenchima, rich in interstitial vascularization; in perinatal period is collapsed
Little bronchi and bronchioli are narrow and are deficient in connective and muscular tissue – they are easily collapsed and obstructed
Inadequate drainage of several segments due to peculiarities of bronchial branching – frequent involvement of I, II, IX, X, VI segments bilateral and of IV, V segments of left lung
Lack of elastic fibers and surfactant –lung rigidity, inclination to atelectasis and emphysema development
Insufficient mucocilliar clearance – difficulties in foreign bodies removing
Insufficient synthesis of interferon and IgA – incompatibility immune response
Plethoric lung parenchima, rich in interstitial vascularization; in perinatal period is collapsed

Слайд 5Predisposing premorbid factors for pneumonia
Premature newborns
Severe perinatal pathology: prenatal hypoxia,
asphyxia, intrapartum trauma
Vomiting and regurgitation syndrome
Artificial feeding
Constitution anomalies
Rickets
Malnutrition
Congenital heart diseases
Cystic fibrosis
Congenital lung malformations
Surgical treatment
Inherited immunodeficiencies
Hypovitaminosis
Chronic focuses of infection
Smoking
Vomiting and regurgitation syndrome
Artificial feeding
Constitution anomalies
Rickets
Malnutrition
Congenital heart diseases
Cystic fibrosis
Congenital lung malformations
Surgical treatment
Inherited immunodeficiencies
Hypovitaminosis
Chronic focuses of infection
Smoking

Слайд 6Pneumonia etiology
Streptococcus Pneumonia ( 60-80% cases of community acquired pneumonia
Hemophilus influenzae
Moraxella
Catarrhalis
In newborns and infants – Staphylococcus, gram (-) microflora
Mycoplasma pneumonia, Chlamidia psittaci, Chl.pneumonia (10-12%).
Severe pneumonia are caused by mixed micriflora
Pneumocystis pneumonia can develop only in immune compromised host (deep prematurity, combined immunodefficiancy, AIDS, imunosuppression)
Viral pneumonia is rare disease. It can be caused by flu, (hemorrhagic pneumonia,), in bronchiolitis, adenoviral and RS viral infection
In newborns and infants – Staphylococcus, gram (-) microflora
Mycoplasma pneumonia, Chlamidia psittaci, Chl.pneumonia (10-12%).
Severe pneumonia are caused by mixed micriflora
Pneumocystis pneumonia can develop only in immune compromised host (deep prematurity, combined immunodefficiancy, AIDS, imunosuppression)
Viral pneumonia is rare disease. It can be caused by flu, (hemorrhagic pneumonia,), in bronchiolitis, adenoviral and RS viral infection

Слайд 7All microorganisms from sputum are divided into 3 groups
pathogenic
provisional pathogenic
nonpathogenic

Слайд 8Pathogenic are microorganisms with complementary receptors to surface cell receptors in
respiratory tract. It gives them opportunity to adhere and multiply on mucus membrane of respiratory tract.
They are Pneumococcus, Hemophylus influenza, Legionella, Mycoplasma, Ricketsia, Mycobacterium tuberculosis etc.
Provisional pathogenic are microorganisms that have no receptors and can’t be fixed on epithelium. Protective mechanisms can easily eliminate them. Only impairment of these mechanisms lead for their penetration, spreading and multiplying ( ARD, overcooling, immune suppression etc)
Nonpathogenic microbes –microorganisms that can cause inflammation only in cases of severe degree of immunodeficiency. They are aerobe and anaerobe saprophytes from upper respiratory tract.

Слайд 9Diagnostic criteria of bacterial pneumonia
Anamnestic data
Hospital acquired pneumonia is developed in
48 hours after hospitalization and 48 h after discharging from hospital
Bacterial intoxication symptoms
Clinical:
Fever more than 3 days
Tachycardia
Paleness, regurgitation
Lab data:
Neutrophyl leukocytosis
Elevated ESR
Functional respiratory disturbancies
Increased respiratory rate more than 20% from age norma
Accessory musculature involving in respiration
Cough or its equivalents
Cyanosis ( perioral, periorbital, diffuse)
Local symptoms in pneumonia:
Percussion sound shortening ( dullness)
Breathing sound conductivity changes (attenuation, rales)
Radiologic confirmation
Bacterial intoxication symptoms
Clinical:
Fever more than 3 days
Tachycardia
Paleness, regurgitation
Lab data:
Neutrophyl leukocytosis
Elevated ESR
Functional respiratory disturbancies
Increased respiratory rate more than 20% from age norma
Accessory musculature involving in respiration
Cough or its equivalents
Cyanosis ( perioral, periorbital, diffuse)
Local symptoms in pneumonia:
Percussion sound shortening ( dullness)
Breathing sound conductivity changes (attenuation, rales)
Radiologic confirmation


Слайд 11Focal pneumonia (30-40% of pneumonia)
It frequently starts from bronchi – bronchopneumonia
Frequently
developed after ARD
Cough is deep and moist
Intoxication
Respiratory failure can be present
Percussion pulmonary clear sound or even with resonance sound but under the focus shortening of the sound
Auscultation: focal bubbling rales, focal crepitation
If accompanied by bronchitis – bilateral dry and moist rales
Radiologic picture presence of interstitial involvement with focal infiltration of 1,5 cm in diameter
More younger the child more frequently affected upper lobes
Cough is deep and moist
Intoxication
Respiratory failure can be present
Percussion pulmonary clear sound or even with resonance sound but under the focus shortening of the sound
Auscultation: focal bubbling rales, focal crepitation
If accompanied by bronchitis – bilateral dry and moist rales
Radiologic picture presence of interstitial involvement with focal infiltration of 1,5 cm in diameter
More younger the child more frequently affected upper lobes
It frequently starts from bronchi – bronchopneumoniaFrequently developed after ARDCough is")
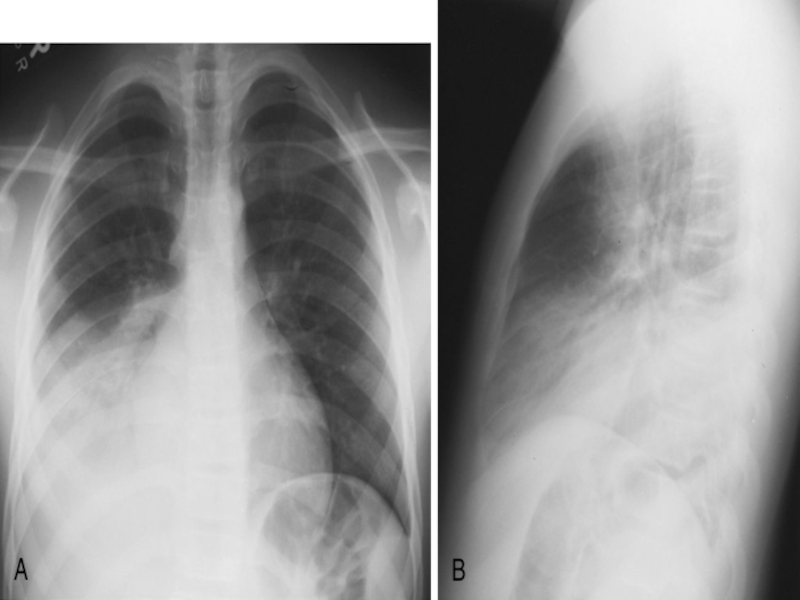
Слайд 12Focal-confluent pneumonia
Several segments are affected or the whole lobe with focal
pulmonary destruction. Intoxication is prominent, massive lung tissue involvement, usually pleurisy.
As a rule ARD precedes with progressive course with involvement of bronchi.
Radiologic peculiarities
Infiltrative shadows are not homogeneous
Process usually is unilateral more frequently in right lung
At affected side intercostal and lobe pleura reaction is present
Reaction of lymphnodes is absent as a rule
As a rule ARD precedes with progressive course with involvement of bronchi.
Radiologic peculiarities
Infiltrative shadows are not homogeneous
Process usually is unilateral more frequently in right lung
At affected side intercostal and lobe pleura reaction is present
Reaction of lymphnodes is absent as a rule

Слайд 13Segmental Pneumonia
Pneumonia affects one or several segments. Moist rales are not
typical or they disappear very quickly.
There are 3 types of course:
With good prognosis, without symptoms
Course is like in croupous pneumonia – sudden onset with fever and cyclic course. Pains in abdomen and chest
Clinical picture like in focal pneumonia, but auscultative data are vague, percussion isn’t clear. Frequent pleuricy, atelectasis
Inclination for abscess formation, destruction, lingering course
X-ray signs: more frequent localization in 1,3 segments of right and 8, 9, 10 segments of both lungs, in 5,4 segments of left lung
Process is unilateral as a rule
Regional lymph nodes are increased on affected side
Pleural ( costal or interlobular) reaction is visible
Duration of pneumonia 10-12 days
More frequent complications : atelectasis, pleuritis, destruction
There are 3 types of course:
With good prognosis, without symptoms
Course is like in croupous pneumonia – sudden onset with fever and cyclic course. Pains in abdomen and chest
Clinical picture like in focal pneumonia, but auscultative data are vague, percussion isn’t clear. Frequent pleuricy, atelectasis
Inclination for abscess formation, destruction, lingering course
X-ray signs: more frequent localization in 1,3 segments of right and 8, 9, 10 segments of both lungs, in 5,4 segments of left lung
Process is unilateral as a rule
Regional lymph nodes are increased on affected side
Pleural ( costal or interlobular) reaction is visible
Duration of pneumonia 10-12 days
More frequent complications : atelectasis, pleuritis, destruction

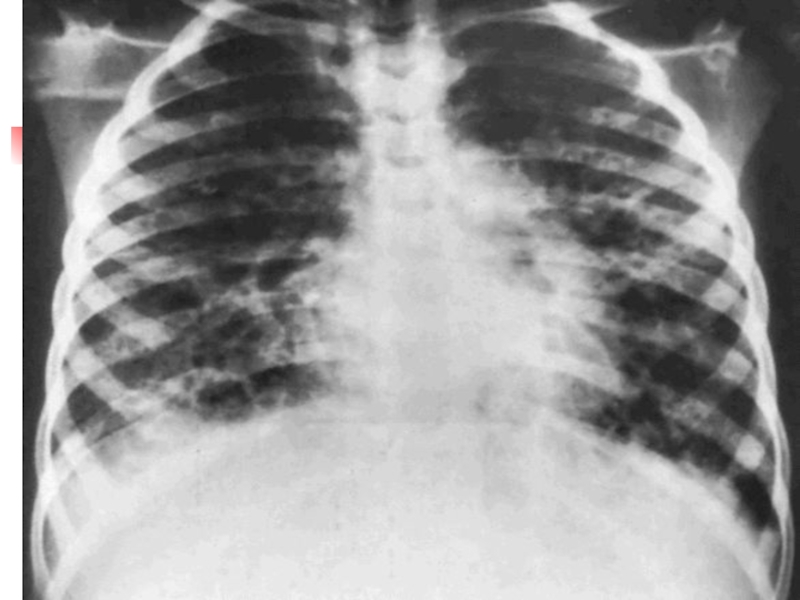
Слайд 14Interstitial pneumonia (1% of all pneumonia)
Acute inflammation of interstitium and less
manifested affection of broncho alveolar structures
Paleness is typical
Pertussis –like cough
Tympanic resonance during percussion
Respiratory sound is rough, irregular dry and various moist bubbling rales
Prominent respiratory failure
Pathogen can’t be revealed in common way
More frequent causative factors are fungus, Pneumocystis, Chlamidia, Mycoplasma, Ricketsia, Legionellas
Paleness is typical
Pertussis –like cough
Tympanic resonance during percussion
Respiratory sound is rough, irregular dry and various moist bubbling rales
Prominent respiratory failure
Pathogen can’t be revealed in common way
More frequent causative factors are fungus, Pneumocystis, Chlamidia, Mycoplasma, Ricketsia, Legionellas
Acute inflammation of interstitium and less manifested affection of broncho")
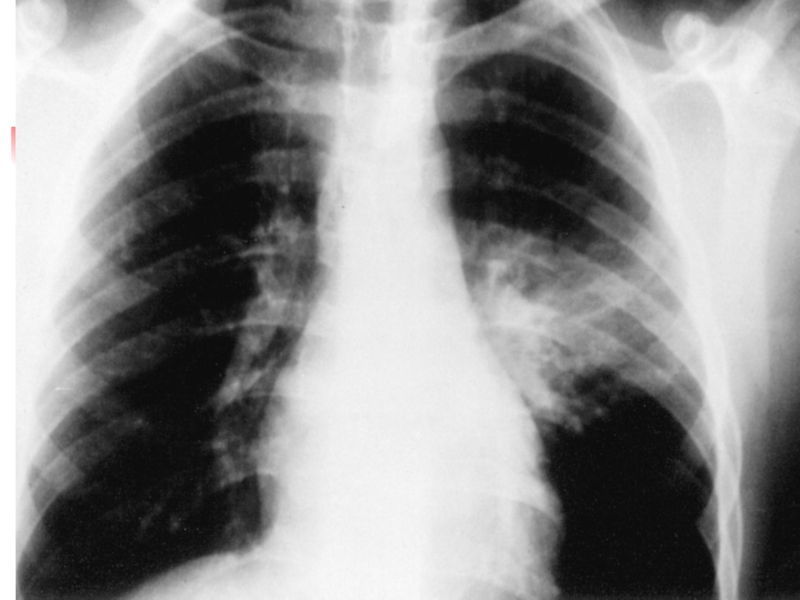
Слайд 15Croupous pneumonia
Classic example of community acquired pneumonia. It is lobe
or
segment affection with pleura involvement (pleuropneumonia).
It’s difficult to differ it from segmental pneumonia only
radiologically. Clinical picture plays the clue role
Acute onset
Cyclic course
Febrile or high febrile fever, flush red on affected side
Sputum is rusty, herpes labialis and nasalis
Lung destruction is very rare
Localization in lower lobes
Chest pain due to pleuritis
Abdomen pain like in appendicitis
Meningeal form of pneumonia
It’s difficult to differ it from segmental pneumonia only
radiologically. Clinical picture plays the clue role
Acute onset
Cyclic course
Febrile or high febrile fever, flush red on affected side
Sputum is rusty, herpes labialis and nasalis
Lung destruction is very rare
Localization in lower lobes
Chest pain due to pleuritis
Abdomen pain like in appendicitis
Meningeal form of pneumonia

Слайд 16Respiratory Failure –is a condition of disturbed gaseous blood composition due
to lung function failure or when maintaining of proper partial O2 and CO2 containing is achieved by forcing of external respiratory structures that produce functional exhaustion of organism.

Слайд 17Clinical classification of respiratory failure
Grade I
Dyspnea after loading, in rest
dyspnea is absent. Accessory musculature
isn’t involved, irregular perioral cyanosis more visible after agitation. BP is
normal. HR ratio to RR=3,5-2,5 : 1`, tachycardia. Blood gases composition: PaCO2 <4,67 Kpa : Pa O2=8,76-10 kPa
Grade II
Dyspnea in rest, accessory musculature involvement, retractions in chest,
constant acrocyanosis, BP is elevated, tachycardia, flaccidity, drowsiness,
adynamia. HR ratio RR = 2-1,5 : 1: PaO2= 7,33-8,53 kPa: PaCO2 = 4,67-5,87 kPa
Grade III
Manifested dyspnea ( more than 50% from N). Bradypnoe and dyspnoe,
generalized cyanosis, paleness, marmour discoloration of skin.
Somnolence, muscular hypotonia, convulsions, coma. BP decreased HR
ratio RR is intermittent. Pa O2< 5,33 kPa, PaCO2> 9,87 kPa
isn’t involved, irregular perioral cyanosis more visible after agitation. BP is
normal. HR ratio to RR=3,5-2,5 : 1`, tachycardia. Blood gases composition: PaCO2 <4,67 Kpa : Pa O2=8,76-10 kPa
Grade II
Dyspnea in rest, accessory musculature involvement, retractions in chest,
constant acrocyanosis, BP is elevated, tachycardia, flaccidity, drowsiness,
adynamia. HR ratio RR = 2-1,5 : 1: PaO2= 7,33-8,53 kPa: PaCO2 = 4,67-5,87 kPa
Grade III
Manifested dyspnea ( more than 50% from N). Bradypnoe and dyspnoe,
generalized cyanosis, paleness, marmour discoloration of skin.
Somnolence, muscular hypotonia, convulsions, coma. BP decreased HR
ratio RR is intermittent. Pa O2< 5,33 kPa, PaCO2> 9,87 kPa

Слайд 18Main principles of pneumonia treatment
Treatment must be opportune and integrated
Etiotropic
therapy directed for eradication of pathogen
Treatment of pathologic syndromes, complications and co-morbidities
Rational rehabilitation process
Treatment of pathologic syndromes, complications and co-morbidities
Rational rehabilitation process

Слайд 19Indications for hospitalization
Infants
Respiratory failure, necessity of oxygen therapy, manifested intoxication
Dehydration,
impossibility of oral drinking
Unfavourable premorbid condition, immune deficiency, developmental anomalies
Suspicion as for Staphylococcal etiology, complications like pleuritis. Ineffective home treatment within 24-36 hours
Inability to organize effective home treatment
Unfavourable premorbid condition, immune deficiency, developmental anomalies
Suspicion as for Staphylococcal etiology, complications like pleuritis. Ineffective home treatment within 24-36 hours
Inability to organize effective home treatment

Слайд 20Pay attention for
Respiratory rate ( main index). In children 2-12
mo old RR> 50/min and for children 12 mo- 5 y.o RR>40/min is threatening.
Retractions of chest lower part
Stridor
Retractions of chest lower part
Stridor
. In children 2-12 mo old")
Слайд 21It’s important
Air humidification in room where child is present
Clothes must be
suitable, surrounding temperature must be optimal
Main task is normalization of nose passage of air
Sleeping must be organized with raised head part of bed
Parents mustn’t prohibit child to cough
To provide with proper intake of liquids intake by oral or parenteral way
Feeding must be usual for age enriched by vitamins
Main task is normalization of nose passage of air
Sleeping must be organized with raised head part of bed
Parents mustn’t prohibit child to cough
To provide with proper intake of liquids intake by oral or parenteral way
Feeding must be usual for age enriched by vitamins

Слайд 22Etiotropic therapy
Foundation of etiotropic treatment is empiric start antibiotic therapy with
following its correction
Empiric start antibacterial therapy is performed depending on expected causative factor
Empiric start antibacterial therapy is performed depending on expected causative factor

Слайд 23Main groups of antimicrobial drugs
Beta-lactams
1. Penicillines
2. Cephalosporines
3. Monobactams (Aztreonam)
4. Carbapenems (Imipenem,
Meropenem)
Aminoglycosides
Fluoroquinolones
Macrolides
Glycopeptides
Nitromidazolines
Tetracyclines
Chloramphenicol
Lyncosamines
Nitrophuranes
Sulfanilamides
Antituberculosis
Antifungal
Aminoglycosides
Fluoroquinolones
Macrolides
Glycopeptides
Nitromidazolines
Tetracyclines
Chloramphenicol
Lyncosamines
Nitrophuranes
Sulfanilamides
Antituberculosis
Antifungal
4. Carbapenems (Imipenem, Meropenem)AminoglycosidesFluoroquinolonesMacrolidesGlycopeptidesNitromidazolinesTetracyclinesChloramphenicolLyncosaminesNitrophuranes SulfanilamidesAntituberculosisAntifungal")
Слайд 24Main statements of antibiotic therapy
Antibiotic administration must peroral in community acquired
uncomplicated pneumonia
In case of severe course only parenteral antibiotic administration, combinations of antibiotics
Ineffectiveness of beta-lactams indicate resistant or atypical microorganisms presence
Duration of uncomplicated community acquired pneumonia is 7-10 days. In case of complications duration must be not less than 14 days
In case of parenteral antibiotic administration condition improvement demand change antibiotic administration for oral intake so called step approach
First antibiotic course mustn’t combined with antifungal drugs
In case of severe course only parenteral antibiotic administration, combinations of antibiotics
Ineffectiveness of beta-lactams indicate resistant or atypical microorganisms presence
Duration of uncomplicated community acquired pneumonia is 7-10 days. In case of complications duration must be not less than 14 days
In case of parenteral antibiotic administration condition improvement demand change antibiotic administration for oral intake so called step approach
First antibiotic course mustn’t combined with antifungal drugs

Слайд 25Efficacy criteria of antibiotic therapy in pneumonia
Efficacy assessment is performed in
uncomplicated pneumonia 24-48 hours after treatment beginning. If there are some complications it is performed 48-72 hours later
Main criteria:
Dynamics of common child’s condition
Disappearing of fever
Normalization of respiratory rate and Ps and their ratio
Improving of lab and X-ray data
Main criteria:
Dynamics of common child’s condition
Disappearing of fever
Normalization of respiratory rate and Ps and their ratio
Improving of lab and X-ray data

Слайд 26Effects of antibiotic therapy
Complete effect- temperature decreasing less than 38C 24-48
hours later in uncomplicated pneumonia form or 72 hours later in complicated pneumonia, improving of condition, appetite, dyspnea reducing
Partly improving- temperature is higher 38C with toxicosis resolving, appetite improving, absence of negative radiologic dynamics
Effect absence – Constant high temperature more than 38 C, condition worsening and/or progressive worsening of lung and pleura changes
Partly improving- temperature is higher 38C with toxicosis resolving, appetite improving, absence of negative radiologic dynamics
Effect absence – Constant high temperature more than 38 C, condition worsening and/or progressive worsening of lung and pleura changes


Слайд 28Pathogenic treatment
Respiratory supplementation according to respiratory failure
Desintoxication. If indications are
present intravenous infusion is performed to correct acidic – basic condition, fluid and electrolyte disorders
Symptomatic treatment can include antipyretics etc.
Symptomatic treatment can include antipyretics etc.

")
Слайд 30Questions
To indicate etiologic and pathophysiologic factors at pneumonia in children
To classify
pneumonia, respiratory failure, analyze typical clinic of the pneumonia, respiratory failure in children.
To indicate aspects of the pneumonia in newborns and to mace previous diagnose.
To make list of the examination and to analyze data of the laboratory and instrumental examination.
To prescribe treatment, rehabilitation, prophylaxis of the pneumonia in children.
To diagnose and to give the first medical aim in acute respyratory failure in children.
To perform differential diagnostic of pneumonias in children
To make prognosis at pneumonia.
To demonstrate morally-deontological principles of the subordination in the pulmonologic department
To indicate aspects of the pneumonia in newborns and to mace previous diagnose.
To make list of the examination and to analyze data of the laboratory and instrumental examination.
To prescribe treatment, rehabilitation, prophylaxis of the pneumonia in children.
To diagnose and to give the first medical aim in acute respyratory failure in children.
To perform differential diagnostic of pneumonias in children
To make prognosis at pneumonia.
To demonstrate morally-deontological principles of the subordination in the pulmonologic department