of child infectious diseases
- Главная
- Разное
- Дизайн
- Бизнес и предпринимательство
- Аналитика
- Образование
- Развлечения
- Красота и здоровье
- Финансы
- Государство
- Путешествия
- Спорт
- Недвижимость
- Армия
- Графика
- Культурология
- Еда и кулинария
- Лингвистика
- Английский язык
- Астрономия
- Алгебра
- Биология
- География
- Детские презентации
- Информатика
- История
- Литература
- Маркетинг
- Математика
- Медицина
- Менеджмент
- Музыка
- МХК
- Немецкий язык
- ОБЖ
- Обществознание
- Окружающий мир
- Педагогика
- Русский язык
- Технология
- Физика
- Философия
- Химия
- Шаблоны, картинки для презентаций
- Экология
- Экономика
- Юриспруденция
Transitional states in newborns презентация
Содержание
- 1. Transitional states in newborns
- 2. Fetal Scalp Blood Values during Labor *
- 4. An uncomplicated transition from fetal to newborn
- 9. In contrast with preterm infants, healthy term
- 11. Transient Cutaneous Lesions A number of
- 14. HARLEQUIN COLOR CHANGE Harlequin color change
- 15. ERYTHEMA TOXICUM Erythema toxicum is a
- 17. MILIARIA Miliaria is an eruption resulting
Слайд 1 Transitional states in newborns assistant prof. of Hospital Paediatrics department with course


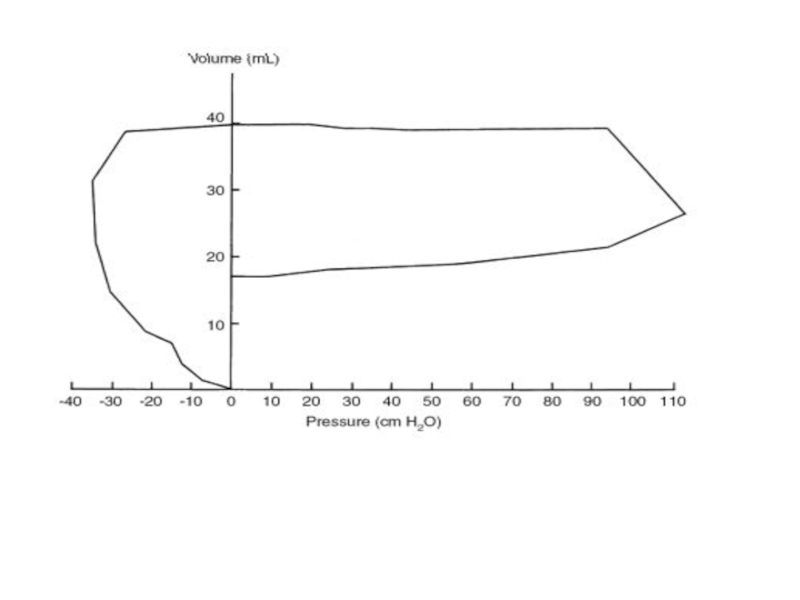
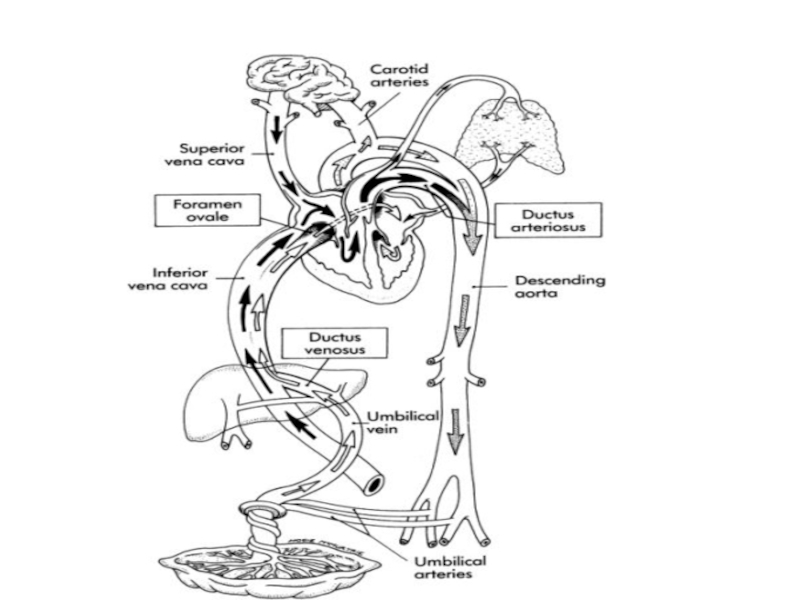
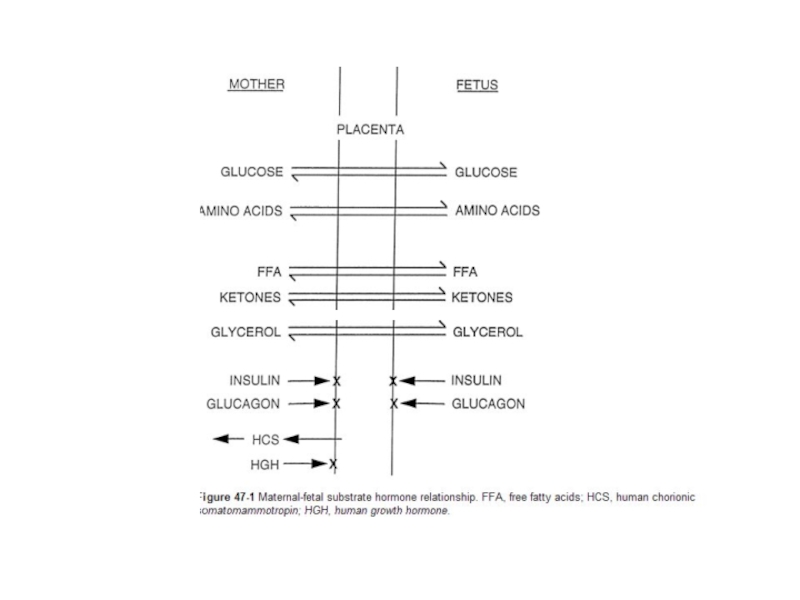
Слайд 4An uncomplicated transition from fetal to newborn status is therefore characterized
by loss of fetal lung fluid, secretion of surfactant, establishment of FRC, a fall in pulmonary vascular resistance, increased systemic pressure after removal of the low-resistance placenta from the systemic circuit, closure of two shunts (the ductus arteriosus and the foramen ovale), and an increase in pulmonary artery blood flow. In most circumstances the mild degree of asphyxia associated with labor is not enough to interfere with this process.
However, the transition may be significantly altered by a variety of antepartum or intrapartum events, resulting in cardiorespiratory depression, asphyxia, or both.
However, the transition may be significantly altered by a variety of antepartum or intrapartum events, resulting in cardiorespiratory depression, asphyxia, or both.

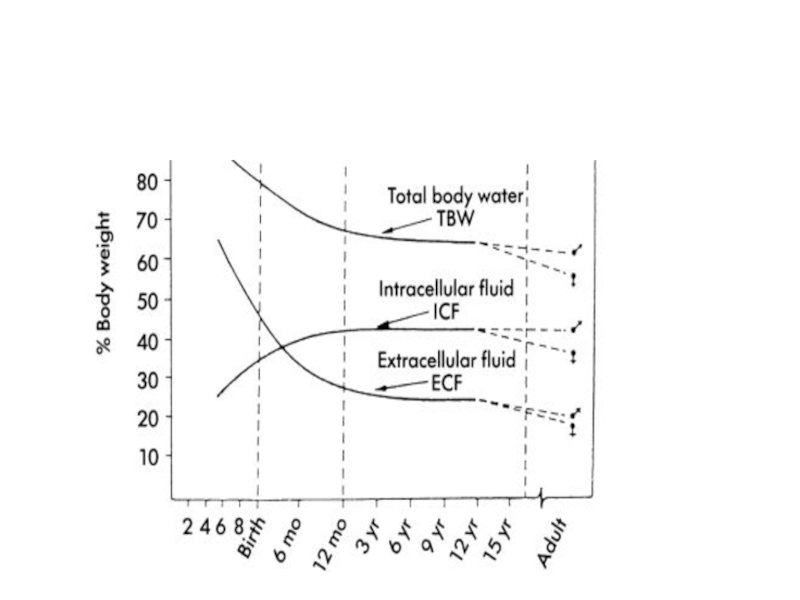
Слайд 9In contrast with preterm infants, healthy term neonates have basal sodium
handling similar to that of adults.
Their FENa is less than 1%, although a transient increase in FENa occurs during the diuretic phase that occurs on the second and third days of life.
Their FENa is less than 1%, although a transient increase in FENa occurs during the diuretic phase that occurs on the second and third days of life.

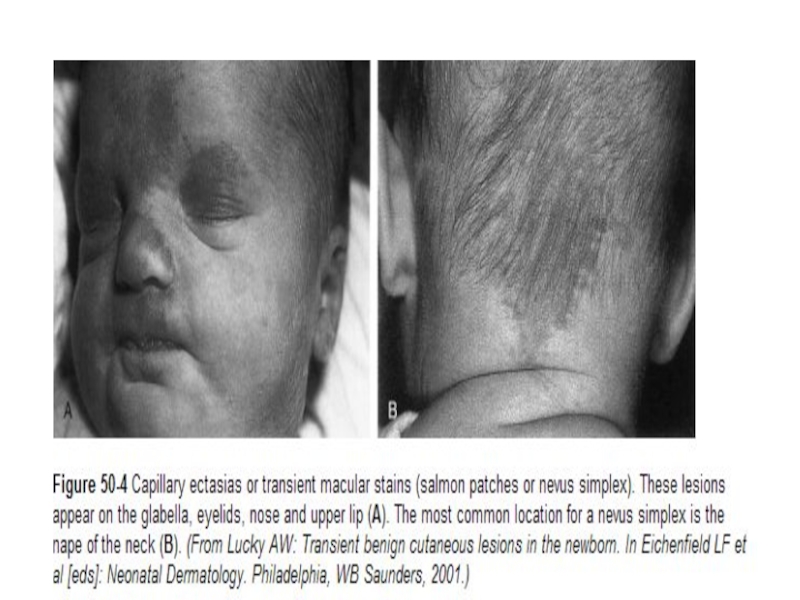
Слайд 11Transient Cutaneous Lesions
A number of benign and transient lesions of
the skin are commonly observed in a normal nursery population.
It is important for the caregiver to distinguish such ephemeral lesions from significant life-threatening diseases with cutaneous manifestations.
It is important for the caregiver to distinguish such ephemeral lesions from significant life-threatening diseases with cutaneous manifestations.


Слайд 14HARLEQUIN COLOR CHANGE
Harlequin color change is a phenomenon observed in
the immediate neonatal period and is more common in the infant with low birthweight. The dependent side of the body becomes intensely red and the upper side pales, with a sharp midline demarcation. The peak incidence of attacks in one series occurred on the second, third, and fourth days, but episodes were observed during the first 3 weeks of life.
These episodes are of no pathologic significance. They have been attributed to a temporary imbalance in the autonomic regulatory mechanism of the cutaneous vessels; there are no accompanying changes in the respiratory rate, muscle tone, or response to external stimuli.
These episodes are of no pathologic significance. They have been attributed to a temporary imbalance in the autonomic regulatory mechanism of the cutaneous vessels; there are no accompanying changes in the respiratory rate, muscle tone, or response to external stimuli.

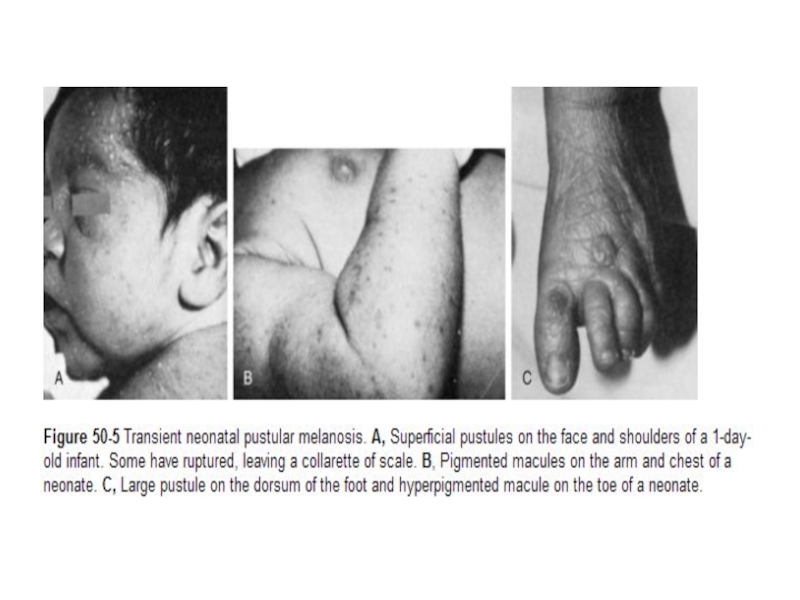
Слайд 15ERYTHEMA TOXICUM
Erythema toxicum is a benign and self-limited eruption that
usually develops between 24 and 72 hours of age, but new lesions can appear until 2 to 3 weeks of age. The disorder is more common in term than in preterm infants, which suggests that it might represent an inflammatory reaction requiring mature skin.
These lesions can vary considerably in character and number; they may be firm, 1- to 3-mm, pale yellow to white papules or pustules on an erythematous base resembling flea bites, or they can be erythematous macules as large as 3 cm in diameter. Individual lesions are evanescent, often lasting only a matter of hours. They may be found on any area of the body but occur only rarely on the palms and soles. They are asymptomatic and have no related systemic involvement.
Their cause is unknown, although a variety of specific cytokines have been implicated in the pathogenesis.[ A microscopic examination of a Wright-stained or Giemsa-stained smear of the pustule contents demonstrates numerous eosinophils; Gram stains are negative for bacteria, and cultures are sterile. No treatment is necessary, because spontaneous resolution occurs in 6 days to 2 weeks.
These lesions can vary considerably in character and number; they may be firm, 1- to 3-mm, pale yellow to white papules or pustules on an erythematous base resembling flea bites, or they can be erythematous macules as large as 3 cm in diameter. Individual lesions are evanescent, often lasting only a matter of hours. They may be found on any area of the body but occur only rarely on the palms and soles. They are asymptomatic and have no related systemic involvement.
Their cause is unknown, although a variety of specific cytokines have been implicated in the pathogenesis.[ A microscopic examination of a Wright-stained or Giemsa-stained smear of the pustule contents demonstrates numerous eosinophils; Gram stains are negative for bacteria, and cultures are sterile. No treatment is necessary, because spontaneous resolution occurs in 6 days to 2 weeks.

Слайд 17MILIARIA
Miliaria is an eruption resulting from eccrine sweat duct obstruction
leading to sweat retention.[38] The three types of lesions are superficial thin-walled vesicles without inflammation (miliaria crystallina); small erythematous, grouped papules (miliaria rubra); and nonerythematous pustules (miliaria pustulosis or profunda).
The eruption most commonly develops in the intertriginous areas and over the face and scalp. It is exacerbated by exposure to a warm and humid environment. Miliaria sometimes can be confused with erythema toxicum; rapid resolution of the lesions when the infant is placed in a cooler environment differentiates them from pyoderma.
A Wright-stained smear of vesicular lesions demonstrates only sparse squamous cells or lymphocytes, permitting exclusion of infectious vesicular eruptions. No topical therapy is indicated.
The eruption most commonly develops in the intertriginous areas and over the face and scalp. It is exacerbated by exposure to a warm and humid environment. Miliaria sometimes can be confused with erythema toxicum; rapid resolution of the lesions when the infant is placed in a cooler environment differentiates them from pyoderma.
A Wright-stained smear of vesicular lesions demonstrates only sparse squamous cells or lymphocytes, permitting exclusion of infectious vesicular eruptions. No topical therapy is indicated.