- Главная
- Разное
- Дизайн
- Бизнес и предпринимательство
- Аналитика
- Образование
- Развлечения
- Красота и здоровье
- Финансы
- Государство
- Путешествия
- Спорт
- Недвижимость
- Армия
- Графика
- Культурология
- Еда и кулинария
- Лингвистика
- Английский язык
- Астрономия
- Алгебра
- Биология
- География
- Детские презентации
- Информатика
- История
- Литература
- Маркетинг
- Математика
- Медицина
- Менеджмент
- Музыка
- МХК
- Немецкий язык
- ОБЖ
- Обществознание
- Окружающий мир
- Педагогика
- Русский язык
- Технология
- Физика
- Философия
- Химия
- Шаблоны, картинки для презентаций
- Экология
- Экономика
- Юриспруденция
Topography of anterolateral abdominal wall презентация
Содержание
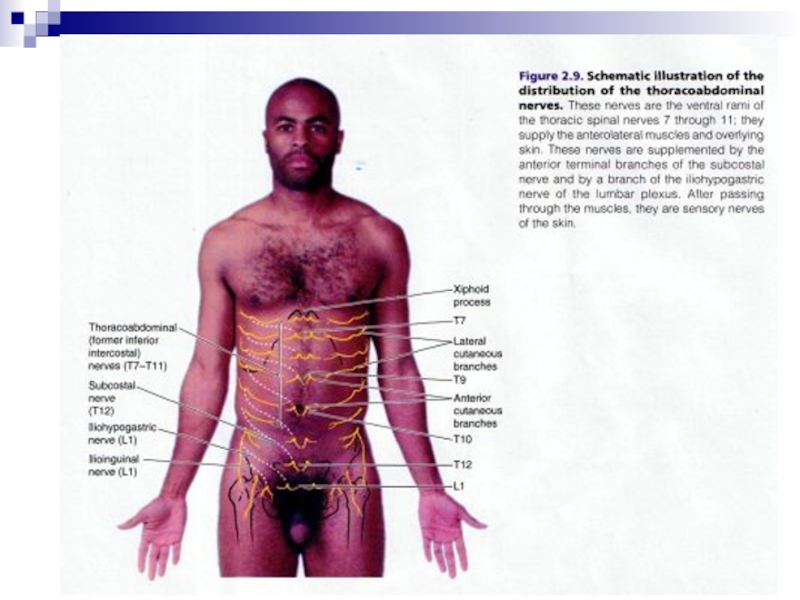
- 1. Topography of anterolateral abdominal wall
- 2. borders
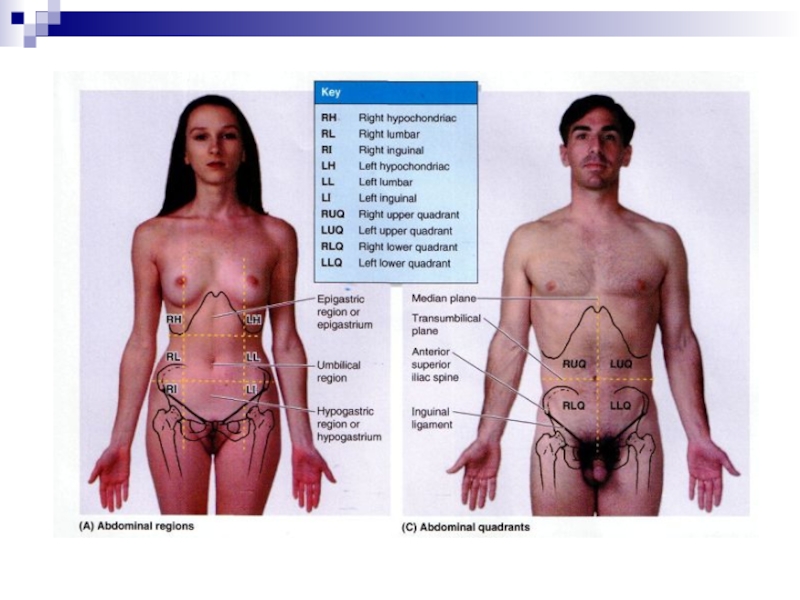
- 4. P243-fig.4.23 Organs’ projection
- 7. Superficial veins subclavian femoral paraumbilical S epigastric S circumflex iliac thoracoepigastric lateral thoracic portal
- 8. Porto-caval anastomoses
- 9. Caput Medusae
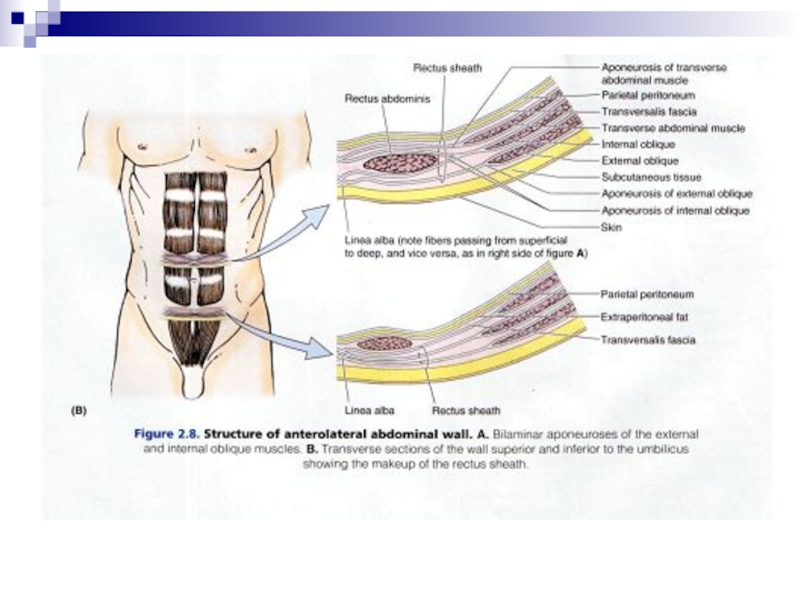
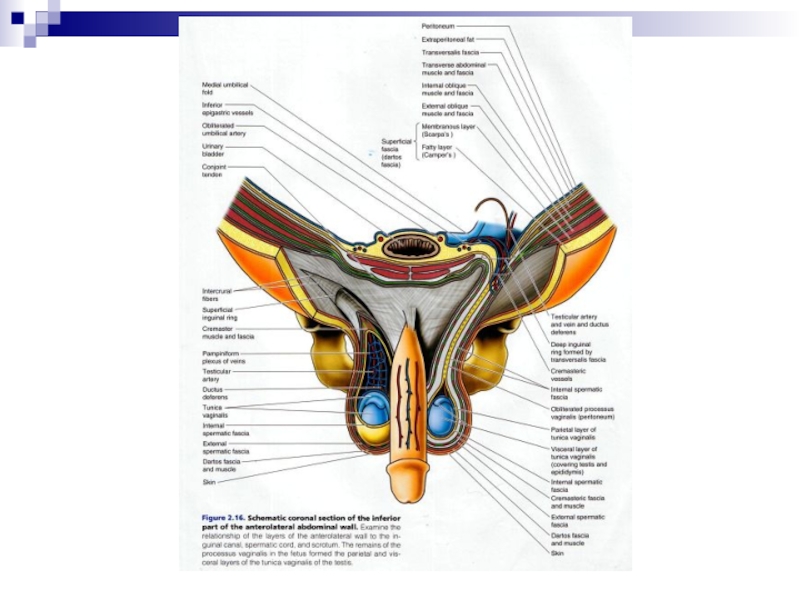
- 15. Fascia superficialis Camper’s fascia Scarpa's fascia P245-fig.4.25~4.26
- 25. A hernia is a protrusion of a
- 26. Parts of hernia
- 27. Types of hernias Inguinal hernia occurs when part
- 28. Hernia types
- 30. Umbilical hernia occurs when fatty tissue or a
- 31. Reducible Hernias When the hernia is
- 32. Irreducible Hernias When a hernia is
- 33. Strangulated Hernias When the hernia is
- 34. Inguinal Hernia Types Direct Inguinal Hernias –
- 37. Clinical presentation contributing factors obesity, chronic
- 38. must examine patient in both supine and
- 39. Treatment surgical: goals are to prevent
- 40. Postoperative complications scrotal hematoma deep bleeding
- 41. Prognosis (inguinal hernia repair) indirect: <
- 42. Intusscusption



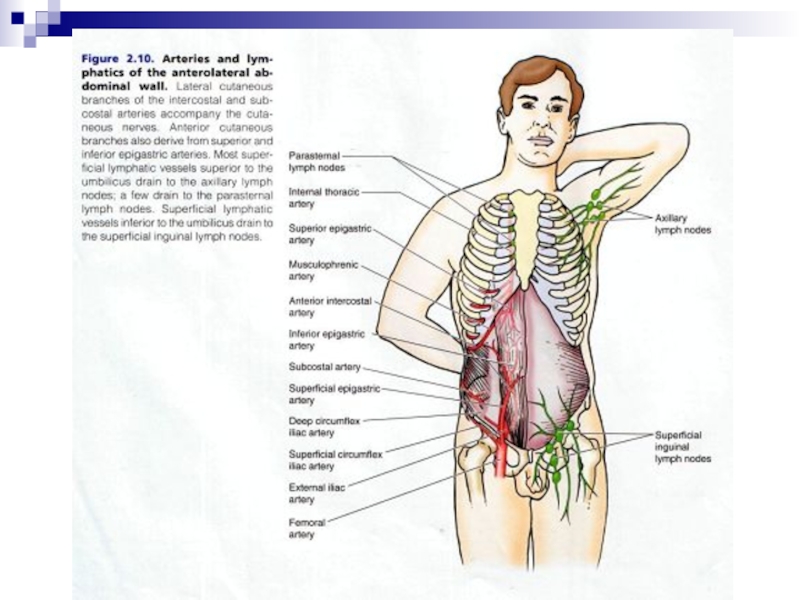
Слайд 7Superficial veins
subclavian
femoral
paraumbilical
S epigastric
S circumflex iliac
thoracoepigastric
lateral thoracic
portal







Слайд 25A hernia is a protrusion of a tissue, structure, or part
of an organ through the muscular tissue or the membrane by which it is normally contained.
A hernia may be likened to a failure in the sidewall of a tire. The tire’s inner tube behaves like the organ and the side wall like the body cavity wall providing the restraint. A weakness in the sidewall allows a bulge to develop allowing the inner tube to protrude leading to the eventual failure of the tire.
A hernia may be likened to a failure in the sidewall of a tire. The tire’s inner tube behaves like the organ and the side wall like the body cavity wall providing the restraint. A weakness in the sidewall allows a bulge to develop allowing the inner tube to protrude leading to the eventual failure of the tire.


Слайд 27Types of hernias
Inguinal hernia occurs when part of bowel (part of digestive
system) pokes through lower abdomen into groin (the area at the front of the body where your thighs meet your abdomen).
Femoral hernia occurs when fatty tissue or a part of bowel pokes through into your groin, at the top of your inner thigh.
Incisional hernia occurs when tissue pokes through a surgical wound in your abdomen that has not fully healed.
Femoral hernia occurs when fatty tissue or a part of bowel pokes through into your groin, at the top of your inner thigh.
Incisional hernia occurs when tissue pokes through a surgical wound in your abdomen that has not fully healed.
 pokes through lower")

Слайд 30Umbilical hernia occurs when fatty tissue or a part of the bowel
pokes through abdomen near navel (belly button).
Hiatus hernia occurs when part of stomach pushes up into chest by squeezing through an opening in the diaphragm (a large, thin sheet of muscle that separates your chest from your abdomen).
Epigastric hernia occurs when fatty tissue pokes through abdomen, between navel and the lower part of your sternum (breastbone).
Spigelian hernia occurs when part of bowel pokes through abdomen at the side of stomach muscle, below your navel.
Muscle hernia occurs when part of muscle pokes through abdomen and can also occur in the muscles in leg, often as the result of a sports injury.
Hiatus hernia occurs when part of stomach pushes up into chest by squeezing through an opening in the diaphragm (a large, thin sheet of muscle that separates your chest from your abdomen).
Epigastric hernia occurs when fatty tissue pokes through abdomen, between navel and the lower part of your sternum (breastbone).
Spigelian hernia occurs when part of bowel pokes through abdomen at the side of stomach muscle, below your navel.
Muscle hernia occurs when part of muscle pokes through abdomen and can also occur in the muscles in leg, often as the result of a sports injury.

Слайд 31Reducible Hernias
When the hernia is reducible it has the ability to
be pushed back inside of the abdominal cavity. This allows people to remove the lump that is showing through and to help control it for a little while.
It is important that you remember that although it is able to be pushed back in this does not repair it. Any straining, coughing, or other movement like this will push the mass right back out. Many people with this type of hernia will wear a special hernia belt to keep it in at all times.
It is important that you remember that although it is able to be pushed back in this does not repair it. Any straining, coughing, or other movement like this will push the mass right back out. Many people with this type of hernia will wear a special hernia belt to keep it in at all times.

Слайд 32Irreducible Hernias
When a hernia is irreducible it means that you do
not have the ability to push the mass back inside of the abdominal cavity. This is probably because the mass is lodged into place and is too large or blocked in by other intestines. Although these might not cause any pain they are uncomfortable. Many people prefer to treat the through surgery as soon as possible to avoid it becoming a strangulated hernia.

Слайд 33Strangulated Hernias
When the hernia is strangulated there is nothing left for
you to do except operate. This is when the hernia has become twisted with an intestine and is cutting off its blood supply. This will cause gangrene and the intestine will die within a few hours if surgery is not performed. This is a very serious condition that can cause an infection and much worse things. Most people will operate before the hernia is able to get to this point.

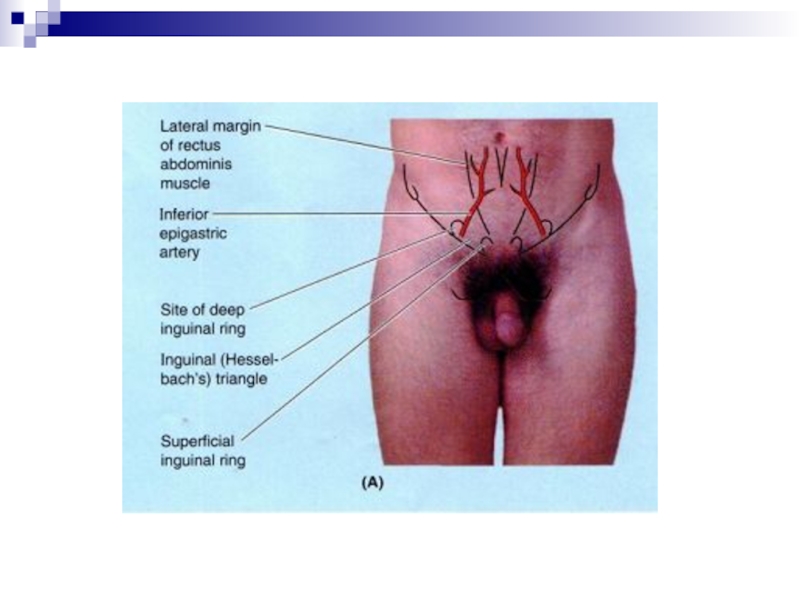
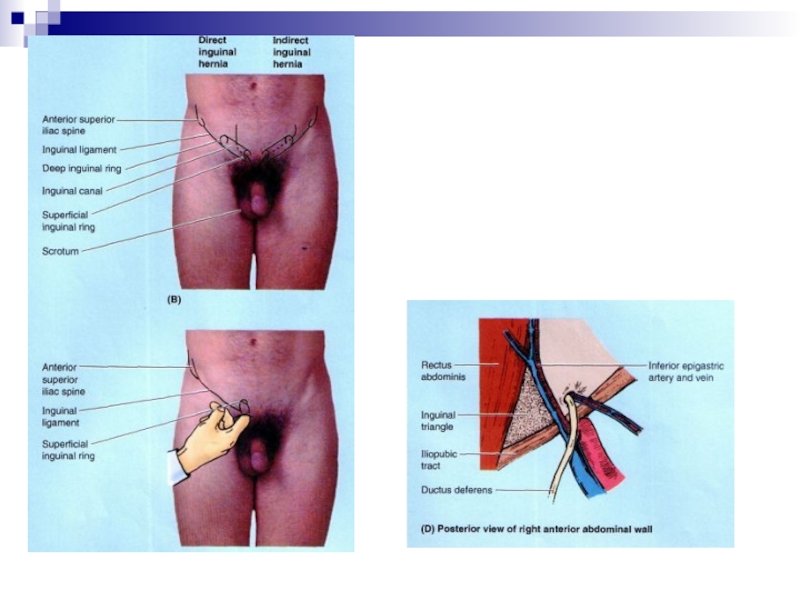
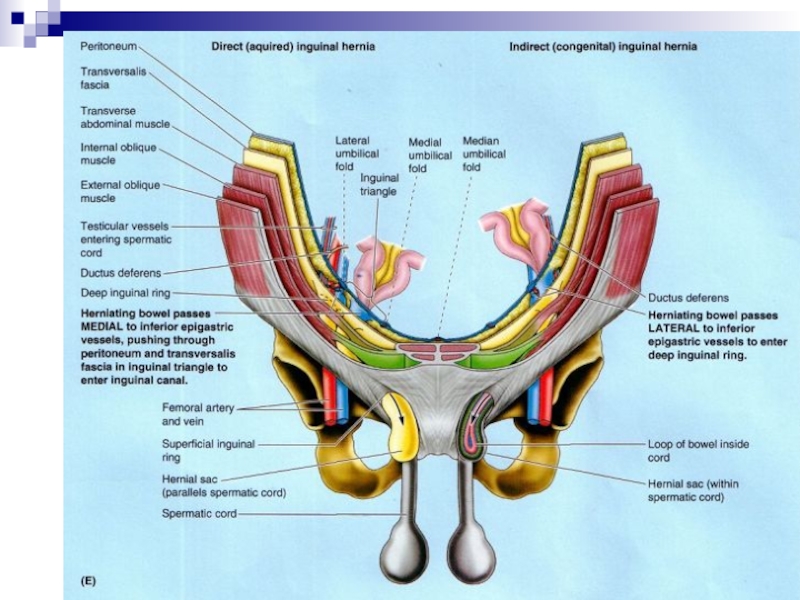
Слайд 34Inguinal Hernia Types
Direct Inguinal Hernias – protrudes through the inguinal ring and
is ultimately the result of the failure of embryonic closure of the internal inguinal ring after the testicle passes through it
Indirect Inguinal Hernias – enters through a weak point in the fascia of the abdominal wall.
An inguinal hernia may also become a strangulated or incarcerated inguinal hernia which is a more serious situation which may involve emergency surgery.
Indirect Inguinal Hernias – enters through a weak point in the fascia of the abdominal wall.
An inguinal hernia may also become a strangulated or incarcerated inguinal hernia which is a more serious situation which may involve emergency surgery.

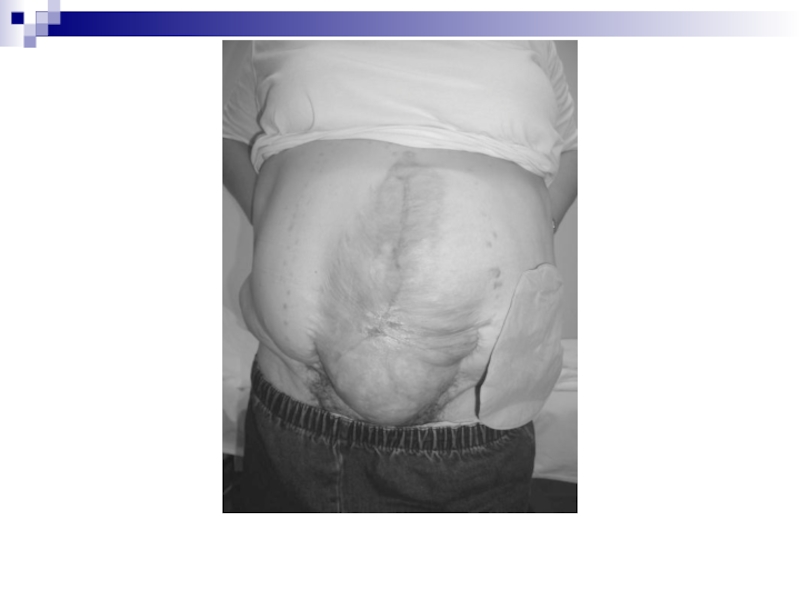
Слайд 37Clinical presentation
contributing factors
obesity, chronic cough, pregnancy, constipation,straining on urination, ascites, activities
which increase intra-abdominal pressure
previous hernia repair
groin mass of variable size
develops insidiously in most cases
occasionally precipitated by single forceful muscular event
associated discomfort
worse at end of day
relieved at night when patient reclines and hernia reduces
relieved with manual reduction
+/- obstruction
+/- local tenderness
previous hernia repair
groin mass of variable size
develops insidiously in most cases
occasionally precipitated by single forceful muscular event
associated discomfort
worse at end of day
relieved at night when patient reclines and hernia reduces
relieved with manual reduction
+/- obstruction
+/- local tenderness

Слайд 38must examine patient in both supine and standing positions
hernial sac and
contents enlarge and transmit palpable impulse when patient coughs or strains
may auscultate bowel sounds
unable to “get above” groin mass with palpation
mass does not transilluminate
strangulation results in
intense pain followed by tenderness
intestinal obstruction
gangrenous bowelsepsis
a surgical emergency
small, new hernias more likely to strangulate
do not attempt to manually reduce hernia if sepsis present or contents of hernial sac thought to be gangrenous
may auscultate bowel sounds
unable to “get above” groin mass with palpation
mass does not transilluminate
strangulation results in
intense pain followed by tenderness
intestinal obstruction
gangrenous bowelsepsis
a surgical emergency
small, new hernias more likely to strangulate
do not attempt to manually reduce hernia if sepsis present or contents of hernial sac thought to be gangrenous

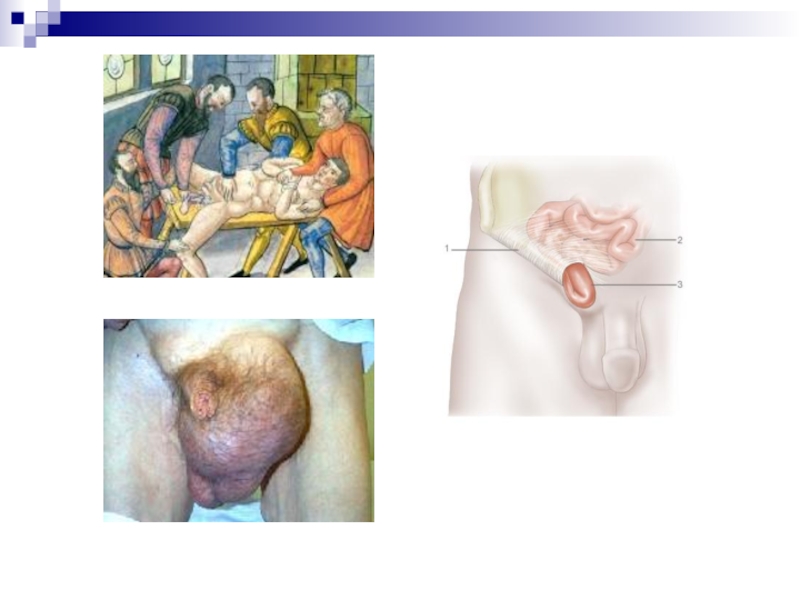
Слайд 39Treatment
surgical: goals are to prevent strangulation, eviscerations
and for cosmetics
indirect hernias -
principle of repair is high ligation of sac and tightening of the internal ring
direct hernias - principle of repair is to rebuild Hesselbach's triangle: need good fascia or a prosthesis
femoral hernias - principle of repair is to remove sac of fat and close the femoral canal with sutures
direct hernias - principle of repair is to rebuild Hesselbach's triangle: need good fascia or a prosthesis
femoral hernias - principle of repair is to remove sac of fat and close the femoral canal with sutures

Слайд 40Postoperative complications
scrotal hematoma
deep bleeding - may enter retroperitoneal space and not
be initially apparent
difficulty voiding
painful scrotal swelling from compromised venous return of testes
neuroma/neuritis
stenosis/occlusion of femoral vein when treating femoral hernias causing acute leg swelling
difficulty voiding
painful scrotal swelling from compromised venous return of testes
neuroma/neuritis
stenosis/occlusion of femoral vein when treating femoral hernias causing acute leg swelling

Слайд 41Prognosis (inguinal hernia repair)
indirect: < 1% risk of recurrence
direct: 3-4% risk
of recurrence
 indirect: < 1% risk of recurrencedirect: 3-4% risk of recurrence")