Development,
Symptoms, Diagnostics, and Treatment.
Measures Preventing the Drug Allergy.
- Главная
- Разное
- Дизайн
- Бизнес и предпринимательство
- Аналитика
- Образование
- Развлечения
- Красота и здоровье
- Финансы
- Государство
- Путешествия
- Спорт
- Недвижимость
- Армия
- Графика
- Культурология
- Еда и кулинария
- Лингвистика
- Английский язык
- Астрономия
- Алгебра
- Биология
- География
- Детские презентации
- Информатика
- История
- Литература
- Маркетинг
- Математика
- Медицина
- Менеджмент
- Музыка
- МХК
- Немецкий язык
- ОБЖ
- Обществознание
- Окружающий мир
- Педагогика
- Русский язык
- Технология
- Физика
- Философия
- Химия
- Шаблоны, картинки для презентаций
- Экология
- Экономика
- Юриспруденция
Drug allergy: the mechanisms of development, symptoms, diagnostics, and treatment. Measures preventing the drug allergy презентация
Содержание
- 1. Drug allergy: the mechanisms of development, symptoms, diagnostics, and treatment. Measures preventing the drug allergy
- 2. Adverse Drug Reactions (ADRs) include all unintended
- 3. Unpredictable reactions: ● Drug Intolerance
- 4. A. Humoral Type: Type I (Anaphylactic) reactions
- 5. B. Cell Mediated: Type IV (Delayed hypersensitivity)
- 6. The antigen reacts with reaginic IgE antibodies,
- 7. DRUG ALLERGY The most dangerous type of
- 8. Allergic Anamnesis Ignoring Analgin,
- 9. The various subtypes of T lymphocytes
- 10. The spectrum of drug allergic reactions and
- 11. Atopic allergy and targets for therapy Allergen
- 12. Aspirin and other NSAIDs are reported to
- 13. Cyclo-oxygenase (COX) and Lipoxygenase (LO) are
- 14. ANTIALLERGIC DRUGS 1. Drugs Stabilizing Mast Cell
- 15. GLUCOCORTICOIDS (GCs) 1. Short-acting: Hydrocortisone acetate
- 16. Mechanism of Action of Glucocorticoids Steroid hormones
- 17. Action of GCs on mediators of inflammatory
- 18. Adverse effects of GCs: Cushing’s syndrome:
- 19. Cromolyn sodium (caps. 20 mg for inhalation)
- 20. Ketotifen (tab. 1 mg), a cromolyn analog,
- 21. H1-Receptors: Exocrine excretion => ?Nasal
- 23. H1-Receptor Antagonists I GENERATION (SEDATIVE): Dimedrol
- 24. Pharmacodynamics of antihistamine H1 blockers ⮞
- 25. Dimedrol (Diphenhydramine)-Tab 0.05 g, amp 1%-1 ml
- 26. Terfenadine (Claritin)-. ● blocks cardiac K+
- 27. Sympathomimetics: Adrenaline h/ch - 0.1% sol. 0.3-0,5-1
- 28. Drugs used to treat Delayed Type Hypersensitivity
- 29. Drugs used to treat Delayed
Слайд 1Zaporizhian State Medical University
Pharmacology Department
Lecture № 3
DRUG ALLERGY: the Mechanisms of

Слайд 2Adverse Drug Reactions (ADRs) include all unintended pharmacologic effects of a
drug except:
● Therapeutic Failures,
● Intentional Overdosage,
● Abuse of the Drug, or
● Errors in Administration.
ADRs are categorized into:
Type A: predictable (75%) – dose dependent, related to the known pharmacologic actions of the drug, and occur in otherwise healthy individuals
Type B: unpredictable (25%) reactions - generally dose independent, unrelated to the actions of
the drug, and occur
only in SUSCEPTIBLE INDIVIDUALS.
● Therapeutic Failures,
● Intentional Overdosage,
● Abuse of the Drug, or
● Errors in Administration.
ADRs are categorized into:
Type A: predictable (75%) – dose dependent, related to the known pharmacologic actions of the drug, and occur in otherwise healthy individuals
Type B: unpredictable (25%) reactions - generally dose independent, unrelated to the actions of
the drug, and occur
only in SUSCEPTIBLE INDIVIDUALS.
 include all unintended pharmacologic effects of a drug except: ● Therapeutic")
Слайд 3Unpredictable reactions:
● Drug Intolerance
● Drug Idiosyncrasy
● Drug
Allergy
● Pseudoallergic Reactions.
Drug allergy is a non-predictable immunologically mediated ADR to a pharmaceutical and/or formulation agent in a sensitized person.
Drug allergy differs from drug toxicity in many ways:
● The lesion produced by allergy is lower in incidence
● It is unpredictable;
● Prior exposure to the drug may cause sensitization;
● The lesion is dose independent and rash, fever,
eosinophilia and blood dyscrasias can occur.
● Pseudoallergic Reactions.
Drug allergy is a non-predictable immunologically mediated ADR to a pharmaceutical and/or formulation agent in a sensitized person.
Drug allergy differs from drug toxicity in many ways:
● The lesion produced by allergy is lower in incidence
● It is unpredictable;
● Prior exposure to the drug may cause sensitization;
● The lesion is dose independent and rash, fever,
eosinophilia and blood dyscrasias can occur.

Слайд 4A. Humoral Type:
Type I (Anaphylactic) reactions - Immediate hypersensitivity reactions are
IgE mediated:
Urticaria, Itching, Subepidermal Necrolysis – Lyell's syndrome, Angioedema, Asthma, Rhinitis, Anaphylactic Shock.
Type II (Cytolytic) reactions are mediated by IgG or IgM:
Blood Transfusion Reactions, Haemolytic Disease of Newborns, Autoimmune Haemolytic Anemia, Thrombocytopenia, Agranulocytosis, Aplastic Anaemia, Haemolysis, Organ Damage (the liver, kidney, muscle), Systemic Lupus Erythematosus and Some Drug Reactions.
Type III (Retarded) reactions are mediated by circulating antibodies (predominantly mopping antibody, IgG):
Serum sickness - symptoms develop within 7-10 days and include Urticaria, Lymphadenopathy, Myalgia, Arthralgia, Fever,
Polyarthritis Nodosa, Stevens-Johnson syndrome.
Systemic lupus erythematosus is an autoimmune disorder that may be induced by Hydralazine, Novocainamide, Isoniazid and other drugs.
Urticaria, Itching, Subepidermal Necrolysis – Lyell's syndrome, Angioedema, Asthma, Rhinitis, Anaphylactic Shock.
Type II (Cytolytic) reactions are mediated by IgG or IgM:
Blood Transfusion Reactions, Haemolytic Disease of Newborns, Autoimmune Haemolytic Anemia, Thrombocytopenia, Agranulocytosis, Aplastic Anaemia, Haemolysis, Organ Damage (the liver, kidney, muscle), Systemic Lupus Erythematosus and Some Drug Reactions.
Type III (Retarded) reactions are mediated by circulating antibodies (predominantly mopping antibody, IgG):
Serum sickness - symptoms develop within 7-10 days and include Urticaria, Lymphadenopathy, Myalgia, Arthralgia, Fever,
Polyarthritis Nodosa, Stevens-Johnson syndrome.
Systemic lupus erythematosus is an autoimmune disorder that may be induced by Hydralazine, Novocainamide, Isoniazid and other drugs.
 reactions - Immediate hypersensitivity reactions are IgE mediated: Urticaria, Itching,")
Слайд 5B. Cell Mediated:
Type IV (Delayed hypersensitivity) reactions:
several hours or days
after exposure to the antigen-
are cell-mediated through production of sensitized
T-lymphocytes carrying receptors for the antigen.
On contact with antigen these T cells produce limphokines which attract granulocytes and generate an inflammatory response, e.g., contact dermatitis, some rashes, fever, photosensitization.
are cell-mediated through production of sensitized
T-lymphocytes carrying receptors for the antigen.
On contact with antigen these T cells produce limphokines which attract granulocytes and generate an inflammatory response, e.g., contact dermatitis, some rashes, fever, photosensitization.
 reactions: several hours or days after exposure to the")
Слайд 6The antigen reacts with reaginic IgE antibodies, bound to the surface
of mast cells and basophils, leading to their degranulation and liberation of histamine and other mediators:
●Those that ⭡Vascular Permeability and contract smooth muscles: Histamine, PAF, SRS-A, Bradykinin.
●Those that are chemotactic for or activate other pro-inflammatory cells: Leukotriene B4,
Eosinophil and Neutrophil Chemotactic Factors.
●Those that modulate the release of other mediators: Bradykinin, PAF, Prostaglandins.
●Those which cause termination of the immune inflammatory response.
●Those that ⭡Vascular Permeability and contract smooth muscles: Histamine, PAF, SRS-A, Bradykinin.
●Those that are chemotactic for or activate other pro-inflammatory cells: Leukotriene B4,
Eosinophil and Neutrophil Chemotactic Factors.
●Those that modulate the release of other mediators: Bradykinin, PAF, Prostaglandins.
●Those which cause termination of the immune inflammatory response.

Слайд 7DRUG ALLERGY
The most dangerous type of ADRs.
45% reports of AR/SE of
drugs in town of Zaporizhia.
900 reports of allergic reactions on drugs
(36% reports of AR/SE of drugs) in Ukraine
during 1996-2008.
Latent forms of hypersensitivity to drugs –
in 10-15% world population and
20% healthy people (according to WHO).
900 reports of allergic reactions on drugs
(36% reports of AR/SE of drugs) in Ukraine
during 1996-2008.
Latent forms of hypersensitivity to drugs –
in 10-15% world population and
20% healthy people (according to WHO).

Слайд 8
Allergic Anamnesis Ignoring
Analgin, Aspirin, Ampicillin were administered in patients with
allergic anamnesis (sometimes with other trade names).
Severe allergic reactions were observed –
Anaphylactic Shock, Quincke‘s edema, Toxic Dermatitis.
Allergic reacitons on Flemoxin and Grunamox in patients with drug allergy to Amoxicillin
Allergic reacitons on Solpadein the active substance of which is Paracetamole.
The main reason of manifestation – absence of knowledge of numerous trade names of
Generic Drugs containing the Same Active Agents.
Severe allergic reactions were observed –
Anaphylactic Shock, Quincke‘s edema, Toxic Dermatitis.
Allergic reacitons on Flemoxin and Grunamox in patients with drug allergy to Amoxicillin
Allergic reacitons on Solpadein the active substance of which is Paracetamole.
The main reason of manifestation – absence of knowledge of numerous trade names of
Generic Drugs containing the Same Active Agents.

Слайд 9The various subtypes of T lymphocytes
(Cytotoxic, Helper and Suppressor) and
their responses constitute Cell Mediated Immunity (CMI).
They regulate Humoral Immunity, B lymphocyte function.
T-cells carrying CD4+ antigen are responsible for
the HELPER function and the delayed hypersensitivity.
Th1 cells enhance CMI but inhibit Humoral Immunity.
Th2 cells have the opposite effect.
T-cells carrying CD8+ antigen are mainly responsible
for the CYTOTOXIC and SUPPRESSOR functions.
They regulate Humoral Immunity, B lymphocyte function.
T-cells carrying CD4+ antigen are responsible for
the HELPER function and the delayed hypersensitivity.
Th1 cells enhance CMI but inhibit Humoral Immunity.
Th2 cells have the opposite effect.
T-cells carrying CD8+ antigen are mainly responsible
for the CYTOTOXIC and SUPPRESSOR functions.
 and their responses constitute Cell")
Слайд 10The spectrum of drug allergic reactions and syndromes
DRESS: Drug Rash with
Eosinophilia and Systemic Symptoms;
TEN - Toxic Epidermal Necrolysis
TEN - Toxic Epidermal Necrolysis

Слайд 11Atopic allergy and targets for therapy
Allergen
Avoid allergen
?
IgE synthesis Desensitize
? Stabilize Mast Cell Membrane
Mast cells Degranulation (Cromolyn, Ketotifen, Ephedrine)
? Mediator Antagonists
Mediator Release (Antihistaminics, Anti-cytokines)
? Late Phase Inhibitors
Local Anaphylaxis (ATOPY) (Glucocorticoids, Indomethacin)
Nose GIT Lungs Skin
(Hay, fever) (Pain, Diarrhea) (Asthma) (Eczema)
?
IgE synthesis Desensitize
? Stabilize Mast Cell Membrane
Mast cells Degranulation (Cromolyn, Ketotifen, Ephedrine)
? Mediator Antagonists
Mediator Release (Antihistaminics, Anti-cytokines)
? Late Phase Inhibitors
Local Anaphylaxis (ATOPY) (Glucocorticoids, Indomethacin)
Nose GIT Lungs Skin
(Hay, fever) (Pain, Diarrhea) (Asthma) (Eczema)

Слайд 12Aspirin and other NSAIDs are reported to account for 21-25% of
all Adverse Drug Reactions
Intake of:
- Analgin
- Diclophenac
- Ketanov
- Baralgetas
produced severe Bronchoobstructive Syndrome in
patients with Aspirin Asthma.
Aspirin-induced asthma refers to the development of acute bronchoconstriction, profuse rhinorrhea and
skin flushing in asthmatic individuals following
the ingestion of aspirin.

Слайд 13Cyclo-oxygenase (COX) and Lipoxygenase (LO) are
2 main pathways of the
metabolism of Arachidonic Acid
The COX pathway converts Arachidonic Acid to Prostaglandins, Prostacyclin and Thromboxane A.
Attacks of asthma precipitated by Aspirin like drugs are due to the inhibition of COX in airways of the sensitive patients:
the Bronchoconstrictor PgF at the expense of
the Bronchodilator PgE2 due to altered COX response.
The LO Pathway converts Arachidonic Acid to
Leukotriene A4 (LT A4) further hydroxylated to LT B4.
LT B4 is a potent chemotactic agent.
The Sulphidopeptide Leukotrienes LT C4, LT D4 and LT E4 are constrictors of the smooth muscle of the airway
Aspirin-induced asthma may relate to the inhibition of COX, resulting in the "shunting" of Arachidonic Acid cascade to the 5- Lipoxygenase pathway.
The COX pathway converts Arachidonic Acid to Prostaglandins, Prostacyclin and Thromboxane A.
Attacks of asthma precipitated by Aspirin like drugs are due to the inhibition of COX in airways of the sensitive patients:
the Bronchoconstrictor PgF at the expense of
the Bronchodilator PgE2 due to altered COX response.
The LO Pathway converts Arachidonic Acid to
Leukotriene A4 (LT A4) further hydroxylated to LT B4.
LT B4 is a potent chemotactic agent.
The Sulphidopeptide Leukotrienes LT C4, LT D4 and LT E4 are constrictors of the smooth muscle of the airway
Aspirin-induced asthma may relate to the inhibition of COX, resulting in the "shunting" of Arachidonic Acid cascade to the 5- Lipoxygenase pathway.
 and Lipoxygenase (LO) are 2 main pathways of the metabolism of Arachidonic AcidThe")
Слайд 14ANTIALLERGIC DRUGS
1. Drugs Stabilizing Mast Cell Membrane:
Glucocorticoids: Prednisolone, Hydrocortisone
Antihistamine H1
: Ketotifen
a Mast cell stabilizer: Cromolyn
β-adrenomimetics: Adrenaline, Ephedrine
Methylxanthines: Euphylline (Aminophylline)
2. Antihistamine H1 agents: Dimedrol, Diprazine, Loratadine
3. Agents eliminating generalized symptoms of immediate allergic reactions:
Adrenomimetics: Adrenaline
Methylxanthines: Euphylline, Theophylline
Ca2+ preparations: Calcium chloride, Ca2+ gluconate
4. Agents decreasing tissue damage: Glucocorticoids
a Mast cell stabilizer: Cromolyn
β-adrenomimetics: Adrenaline, Ephedrine
Methylxanthines: Euphylline (Aminophylline)
2. Antihistamine H1 agents: Dimedrol, Diprazine, Loratadine
3. Agents eliminating generalized symptoms of immediate allergic reactions:
Adrenomimetics: Adrenaline
Methylxanthines: Euphylline, Theophylline
Ca2+ preparations: Calcium chloride, Ca2+ gluconate
4. Agents decreasing tissue damage: Glucocorticoids

Слайд 15GLUCOCORTICOIDS (GCs)
1. Short-acting: Hydrocortisone acetate
Cortisone
2. Intermediate-acting:
Prednisolone
Triamcinolone
3. Long-acting: Betametasone,
Dexametasone
OINTMENTS for local use - Fluorine-containing:
Synaflan, Flumethasone
AEROSOLS or POWDERS FOR INHALATIONS: Beclometasone
Fluticasone
2. Intermediate-acting:
Prednisolone
Triamcinolone
3. Long-acting: Betametasone,
Dexametasone
OINTMENTS for local use - Fluorine-containing:
Synaflan, Flumethasone
AEROSOLS or POWDERS FOR INHALATIONS: Beclometasone
Fluticasone
1. Short-acting: Hydrocortisone acetate Cortisone2. Intermediate-acting: Prednisolone Triamcinolone 3. Long-acting:")
Слайд 16Mechanism of Action of Glucocorticoids
Steroid hormones are lipid soluble and cross
cell membranes easily.
Once inside the cell, the hormone molecules bind with specific receptor proteins.
The hormone–receptor complex enters the nucleus of the cell where it activates Gene Expression –
nucleic acids (DNA and RNA) and
the Genetic Code to synthesize
new proteins.
Once inside the cell, the hormone molecules bind with specific receptor proteins.
The hormone–receptor complex enters the nucleus of the cell where it activates Gene Expression –
nucleic acids (DNA and RNA) and
the Genetic Code to synthesize
new proteins.

Слайд 17Action of GCs on mediators of inflammatory
and immune response:
GCs change
Gene Expression:
? Production of prostanoids owing to
Decreased Expression of COX-2
? Generation of cytokines –
IL 1-6, IL-8, TNF-α and cell adhesion factor – through inhibition of transcription of
the relevant genes
? Complement components in the plasma
? Generation of induced NO
? Histamine release from basophils
? IgG production.
? Production of prostanoids owing to
Decreased Expression of COX-2
? Generation of cytokines –
IL 1-6, IL-8, TNF-α and cell adhesion factor – through inhibition of transcription of
the relevant genes
? Complement components in the plasma
? Generation of induced NO
? Histamine release from basophils
? IgG production.

Слайд 18Adverse effects of GCs: Cushing’s syndrome:
Moon face, with red cheeks
Thin
arms and legs: muscle wasting
?BP, Itracranial Hypertension
Osteoporosis
Cataracts
Thinning of skin
Increased abdominal fat
Buffalo hump
Euphoria
Depression or emotional lability
Avascular necrosis of femoral head
?Appetite, Obesity,
Hyperglycemia, Diabetes
?BP, Itracranial Hypertension
Osteoporosis
Cataracts
Thinning of skin
Increased abdominal fat
Buffalo hump
Euphoria
Depression or emotional lability
Avascular necrosis of femoral head
?Appetite, Obesity,
Hyperglycemia, Diabetes

Слайд 19Cromolyn sodium (caps. 20 mg for inhalation) and
Nedocromil (aerosol: 2
mg/dose) stabilize mast cells and prevent the release of bronchoconstrictive and inflammatory substances when mast cells are confronted with allergens and other stimuli.
They stabilize the mast cell membrane and inhibit release of the mediators of Type I allergic reaction, including: histamine and Slow Reacting Substance of Anaphylaxis (SRS-A) from sensitized must cells.
Pretreatment with cromolyn blocks allergen-induced and exercise-induced bronchoconstriction by acting on inflammatory cells such as eosinophils.
They stabilize the mast cell membrane and inhibit release of the mediators of Type I allergic reaction, including: histamine and Slow Reacting Substance of Anaphylaxis (SRS-A) from sensitized must cells.
Pretreatment with cromolyn blocks allergen-induced and exercise-induced bronchoconstriction by acting on inflammatory cells such as eosinophils.
 and Nedocromil (aerosol: 2 mg/dose) stabilize mast cells")
Слайд 20Ketotifen (tab. 1 mg), a cromolyn analog, is an antihistaminic (H1)
and mast cell stabilizer.
● It inhibits stimulation of immunogenic and inflammatory cells (mast cells, macrophages, eosinophils, lymphocytes, neutrophils) and mediator release.
● It is believed to inhibit airway inflammation induced by
platelet activating factor (PAF).
Ketotifen prevents bronchial asthma attacks.
● It also produces relief in patients with rhinitis, atopic dermatitis, conjunctivitis, urticaria, food allergy, migraine
Adverse effects: sedation, dry mouth, dizziness, nausea,
weight gain.
● It inhibits stimulation of immunogenic and inflammatory cells (mast cells, macrophages, eosinophils, lymphocytes, neutrophils) and mediator release.
● It is believed to inhibit airway inflammation induced by
platelet activating factor (PAF).
Ketotifen prevents bronchial asthma attacks.
● It also produces relief in patients with rhinitis, atopic dermatitis, conjunctivitis, urticaria, food allergy, migraine
Adverse effects: sedation, dry mouth, dizziness, nausea,
weight gain.
, a cromolyn analog, is an antihistaminic (H1) and mast cell stabilizer.")
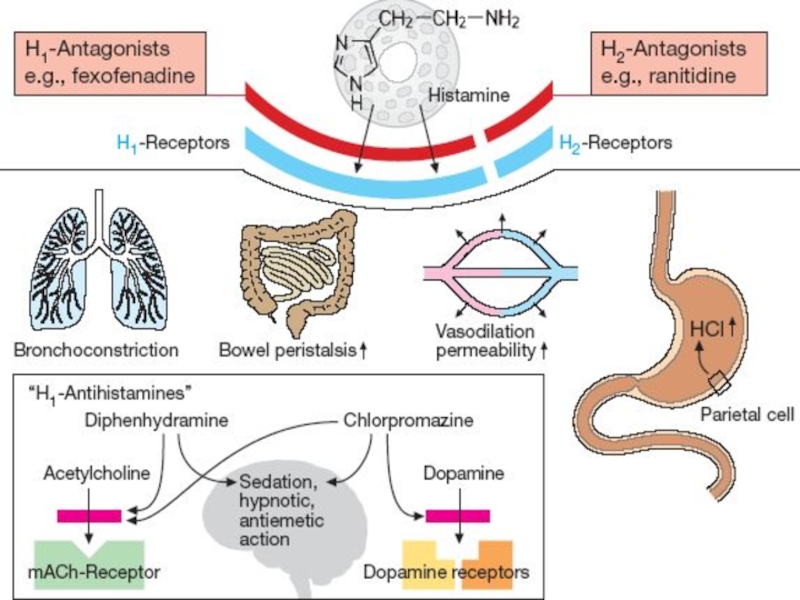
Слайд 21H1-Receptors:
Exocrine excretion => ?Nasal and Bronchial mucus
Bronchial smooth muscle constriction => bronchospasm
Intestinal smooth muscle contraction =>
cramps and diarrhea
Sensory nerve endings: itch and pain
H2-Receptors:
Stomach: Stimulation of Gastric Hydrochloric Acid Secretion
H1- and H2-Receptors:
Cardiovascular system: ?BP and ?HR
Skin:
‘Triple Response’ – Wheal formation, Reddening, Flare
Intestinal smooth muscle contraction =>
cramps and diarrhea
Sensory nerve endings: itch and pain
H2-Receptors:
Stomach: Stimulation of Gastric Hydrochloric Acid Secretion
H1- and H2-Receptors:
Cardiovascular system: ?BP and ?HR
Skin:
‘Triple Response’ – Wheal formation, Reddening, Flare

Слайд 23H1-Receptor Antagonists
I GENERATION (SEDATIVE):
Dimedrol (Diphenhydramine)
Diprazine (Promethazine)
Suprastine (Chloropyramine)
Diazoline
Tavegyl (Clemastin)
II GENERATION
(NON-SEDATIVE):
Loratadine (Claritin)
Terfenadine
Astemizole
Phencarol (Quifenadine)
III GENERATION (ACTIVE METABOLITES):
Telfast (Fexofenadine)
Zirtek (Cetirizine)
Loratadine (Claritin)
Terfenadine
Astemizole
Phencarol (Quifenadine)
III GENERATION (ACTIVE METABOLITES):
Telfast (Fexofenadine)
Zirtek (Cetirizine)
: Dimedrol (Diphenhydramine) Diprazine (Promethazine) Suprastine (Chloropyramine) Diazoline Tavegyl (Clemastin)II GENERATION (NON-SEDATIVE): Loratadine (Claritin)")
Слайд 24Pharmacodynamics of antihistamine H1 blockers
⮞ Block the actions of histamine
by reversible competitive
antagonism at the H1-receptor
⮞ Antagonist effects at other receptors:
⮞ M - Cholinoceptors
⮞ α1 - Adrenoreceptors
⮞ 5-Hydrohytryptamine (5-HT) receptors
Diprazin ⮞ Dimedrol ⮞ Suprastin ⮞ Diazolin
antagonism at the H1-receptor
⮞ Antagonist effects at other receptors:
⮞ M - Cholinoceptors
⮞ α1 - Adrenoreceptors
⮞ 5-Hydrohytryptamine (5-HT) receptors
Diprazin ⮞ Dimedrol ⮞ Suprastin ⮞ Diazolin

Слайд 25Dimedrol (Diphenhydramine)-Tab 0.05 g, amp 1%-1 ml
competes to H1 receptors
on the smooth muscle of
the bronchi, GIT, uterus, and large blood vessels.
By binding to receptors, suppresses histamine-induced allergic symptoms, even though it does not prevent its release.
Central antimuscarinic actions is responsible for antivertigo, antiemetic, and antidyskinetic action.
Clinical uses:
⮞ Allergy symptoms
⮞ Motion sickness
⮞ Parkinson’s disease
⮞ Nonproductive cough
⮞ Insomnia
the bronchi, GIT, uterus, and large blood vessels.
By binding to receptors, suppresses histamine-induced allergic symptoms, even though it does not prevent its release.
Central antimuscarinic actions is responsible for antivertigo, antiemetic, and antidyskinetic action.
Clinical uses:
⮞ Allergy symptoms
⮞ Motion sickness
⮞ Parkinson’s disease
⮞ Nonproductive cough
⮞ Insomnia
-Tab 0.05 g, amp 1%-1 ml competes to H1 receptors on the smooth muscle")
Слайд 26Terfenadine (Claritin)-.
● blocks cardiac K+ channels, prolongs Q-T and
has
occasionally produced Polymorphic Ventricular Tachycardia.
The risk is increased in liver disease or when inhibitors of CYP3A4 are administered concurrently – because larger amounts of unchanged drug reach systemic circulation.
Erythromycin, Clarithromycin, Ketoconazole and Itraconazole
are the drugs precipitating their
cardiotoxicity as they block
microsomal CYP-450 enzymes.
Because of this risk,
Terfenadine has been withdrawn
by most manufactures.
Clinical use: allergic rhinitis
The risk is increased in liver disease or when inhibitors of CYP3A4 are administered concurrently – because larger amounts of unchanged drug reach systemic circulation.
Erythromycin, Clarithromycin, Ketoconazole and Itraconazole
are the drugs precipitating their
cardiotoxicity as they block
microsomal CYP-450 enzymes.
Because of this risk,
Terfenadine has been withdrawn
by most manufactures.
Clinical use: allergic rhinitis
-. ● blocks cardiac K+ channels, prolongs Q-T and has occasionally produced Polymorphic Ventricular")
Слайд 27Sympathomimetics:
Adrenaline h/ch - 0.1% sol. 0.3-0,5-1 ml in 2-3 ml of
0.9% NCl solution SC in the region of injection and around it,
SL or intratracheal instillation,
Mesaton 1% sol. 1-2 ml IV in
0.9% NaCl solution
Noradrenaline h/t 0.2% in
0.9% NCl solution IV infusion
SL or intratracheal instillation,
Mesaton 1% sol. 1-2 ml IV in
0.9% NaCl solution
Noradrenaline h/t 0.2% in
0.9% NCl solution IV infusion
Glucocorticoids:
Prednisolone 3% solution 30-90 mg and more IV
in 0.9% NCl solution
Broncholytics:
Euphylline 2.4% sol.
3-5-10 ml IV
in 0.9% NaCl solution
Oxygen inhalation for hypoxia control or
prevention
Enzyme preparations:
Penicillinase 1000 000 UA in 2 ml of 0.9% NaCl solution in the region of injection
Cardiac Glycosides:
Strophanthine
0.025% 1-2 ml IV in
0.9% NCl solution
Anaphylactic shock

Слайд 28Drugs used to treat Delayed Type Hypersensitivity Reactions:
I. IMMUNOSUPRESSANTS
- suppressing mainly
cell-mediated immunity:
1.Inhibitors of IL-2 production or action:
Cyclosporine (Sandimmune)
Tacrolimus
2.Inhibitors of cytokine gene expression:
Glucocorticoids: Prednisolone
3. Antitumor Cytotoxic Agents:
a) Alkylating agents: Cyclophosphan
b) Antimetabolites: Azathioprine, Mercaptopurine, Methotrexate
4.Blockers of the T-cell surface molecules involved in signaling - Monoclonal Antibodies: Basiliximab and Daclizumab
cell-mediated immunity:
1.Inhibitors of IL-2 production or action:
Cyclosporine (Sandimmune)
Tacrolimus
2.Inhibitors of cytokine gene expression:
Glucocorticoids: Prednisolone
3. Antitumor Cytotoxic Agents:
a) Alkylating agents: Cyclophosphan
b) Antimetabolites: Azathioprine, Mercaptopurine, Methotrexate
4.Blockers of the T-cell surface molecules involved in signaling - Monoclonal Antibodies: Basiliximab and Daclizumab

Слайд 29
Drugs used to treat
Delayed Type Hypersensitivity Reactions:
II. Drugs decreasing
tissue damage –
1. Glucocorticoids
2. NSAIDs
1. Glucocorticoids
2. NSAIDs