- Главная
- Разное
- Дизайн
- Бизнес и предпринимательство
- Аналитика
- Образование
- Развлечения
- Красота и здоровье
- Финансы
- Государство
- Путешествия
- Спорт
- Недвижимость
- Армия
- Графика
- Культурология
- Еда и кулинария
- Лингвистика
- Английский язык
- Астрономия
- Алгебра
- Биология
- География
- Детские презентации
- Информатика
- История
- Литература
- Маркетинг
- Математика
- Медицина
- Менеджмент
- Музыка
- МХК
- Немецкий язык
- ОБЖ
- Обществознание
- Окружающий мир
- Педагогика
- Русский язык
- Технология
- Физика
- Философия
- Химия
- Шаблоны, картинки для презентаций
- Экология
- Экономика
- Юриспруденция
Articular system презентация
Содержание
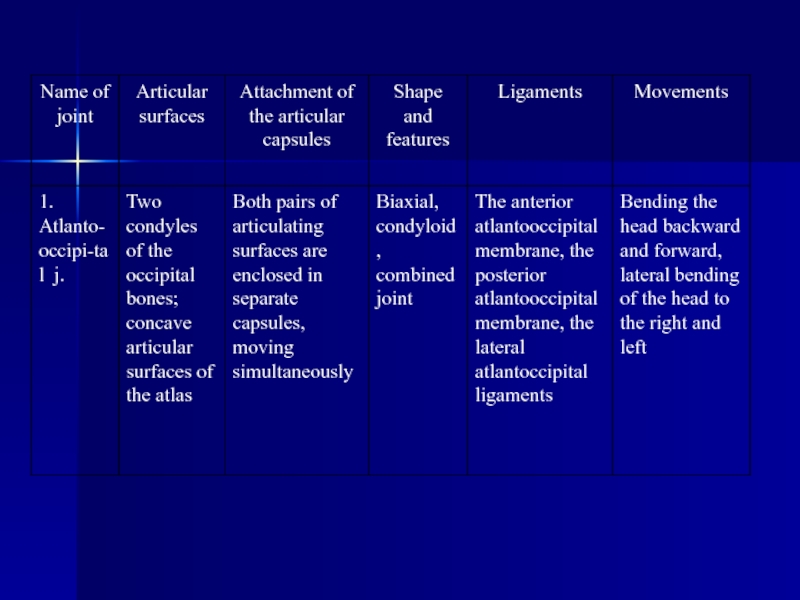
- 1. Articular system
- 2. PLAN: Development of joints. Classification
- 3. Development of joints
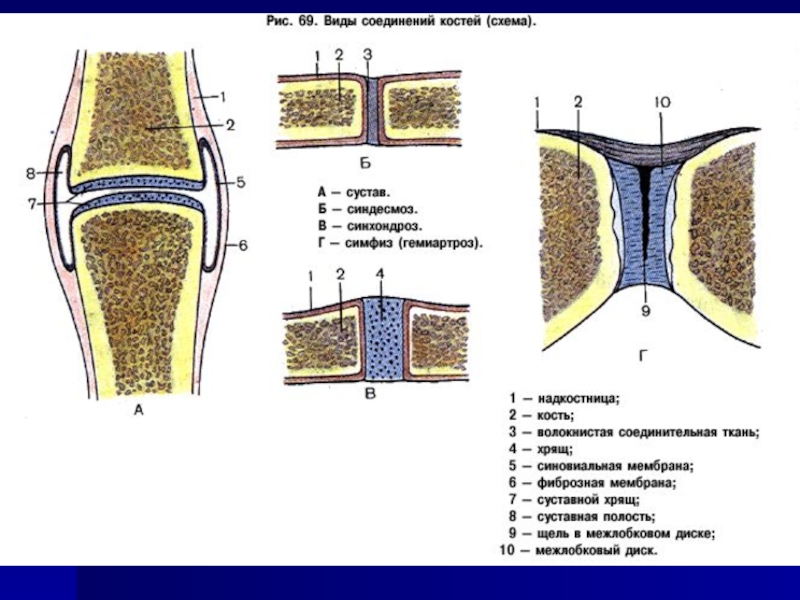
- 4. CLASSIFICATION OF BONE ARTICULATIONS Continuous articulations(synarthroses)
- 5. CONTINUOUS BONE ARTICULATIONS
- 7. Syndesmoses, syndesmosis, (juncturae fibrosae)
- 12. SYNCHONDROSES: ACCORDING TO THE DURATION OF THE
- 15. When
- 16. SYNOVIAL JOINTS
- 17. THE MOST TYPICAL FEATURES OF THE
- 20. Synovial folds and bursae. The synovial
- 22. Factors, which aid in the stabilization of
- 23. Congruent and incongruent joints
- 24. Movements in the joints The frontal axis
- 25. CLASSIFICATION OF JOINTS
- 26. Classification of the joints based on
- 31. Clinical applications
- 53. THE TEMPOROMANDIBULAR JOINT
- 54. Ligaments. The capsule is reinforced
- 55. MASTICATORY MUSCLES The masticatory muscles are derived
- 56. THE DEEP MASTICATORY MUSCLES Medial pterygoid,
- 57. Muscles of the neck Is divided
- 58. Middle muscles of the neck Is divided
- 59. Muscles located below the hyoid bone
- 60. The Deep muscles of the neck Is
- 61. THE END THANK FOR YOUR ATTENTION

Слайд 2PLAN:
Development of joints.
Classification of bone articulations.
Continuous bone articulations.
Synovial joints.
The most typical
Accessory structures of joints.
Congruent and incongruent joints.
Movements in the joints.
Classification of the joints based on the number of articulating surfaces.
Classification of the joints based on the shape of articulating surfaces.
Clinical applications.

Слайд 3Development of joints

Слайд 4CLASSIFICATION OF BONE ARTICULATIONS
Continuous articulations(synarthroses) are characterized by the presence of
Discontinuous (synovial) articulations contain a cavity lined with the synovial membrane. They possess a great mobility. They are called joints.
Intermediate forms between the continuous and discontinuous articulations are symphyses (or hemiarthroses). They are represented by the cartilaginous articulations with the cleft-like cavity lacking a fibrous capsule and without synovial membrane.
 are characterized by the presence of an uninterrupted articulating")
Слайд 5CONTINUOUS BONE ARTICULATIONS
Depending on the
fibrous, syndesmoses,
cartilaginous, synchondroses,
osseous, synostoses.

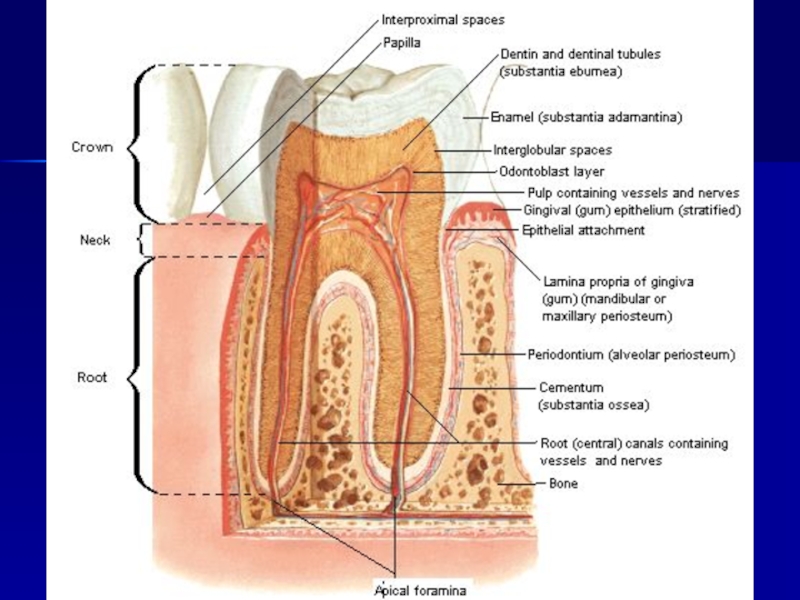
Слайд 7 Syndesmoses, syndesmosis, (juncturae fibrosae) are formed from the
gomphosis, gomphosis, dentoalveolar syndesmosis, a fibrous articulation between the periodontium of alveolar socket and the root of the tooth;
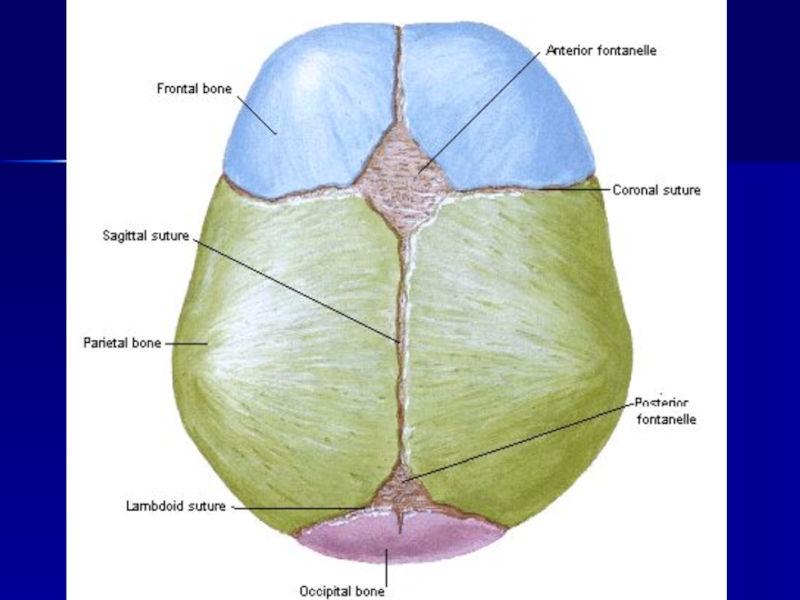
sutures, sutura, fibrous articulations between the bones of the skull, which contain a thin layer of connective tissue;
fontanelles, fonticuli, between bones of skull of the new-born;
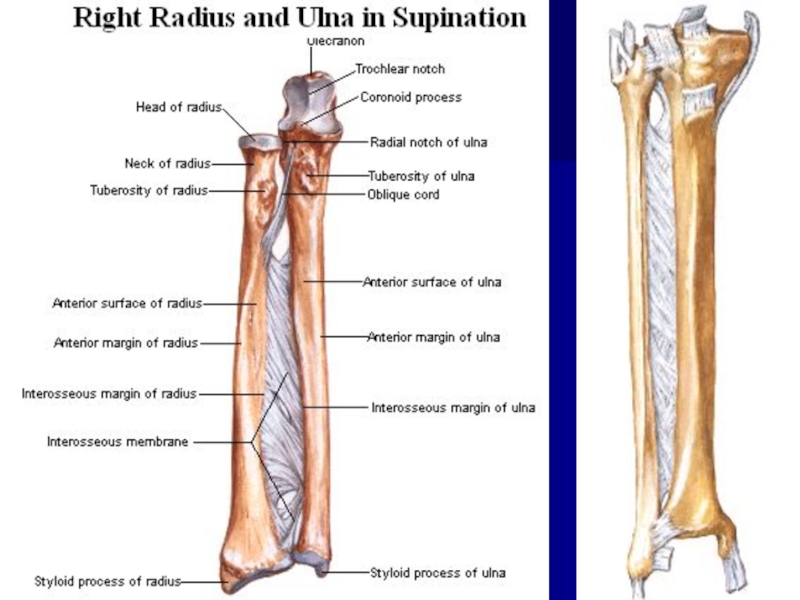
interosseous membranes, membranae interosseae;
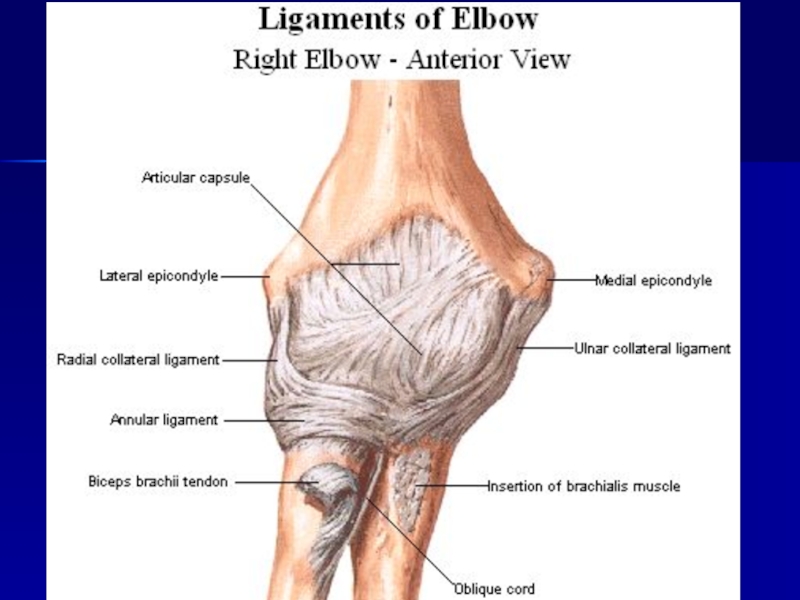
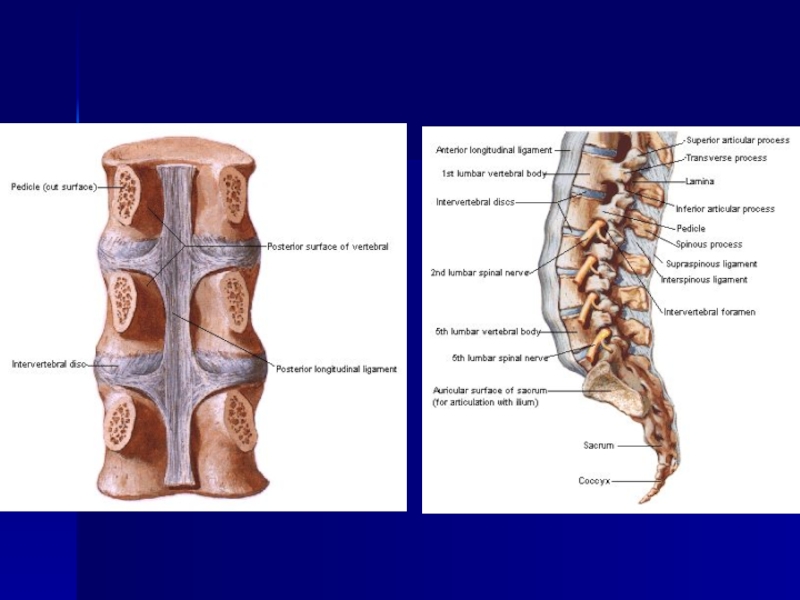
ligaments, ligamenta, most of the ligaments consist of a dense regular connective tissue. Fibers in the ligaments run obliquely and cross over like in the rope. Therefore, ligaments are quite resilient. Collagen fibers of the ligaments, besides resiliency, provide great elasticity. Some ligaments, besides collagen fibers, contain a considerable amount of elastic tissue yellow in color. They are characterized by lower resilience but greater elasticity. They perform a shock-absorbing function (e.g. yellow ligaments of the vertebral column). Because of their low resilience, elastic ligaments are not very common in the body.
 are formed from the fibrous connective tissue and are")
Слайд 12SYNCHONDROSES:
ACCORDING TO THE DURATION OF THE EXISTENCE :
2—PERMANENT— exist throughout the life.
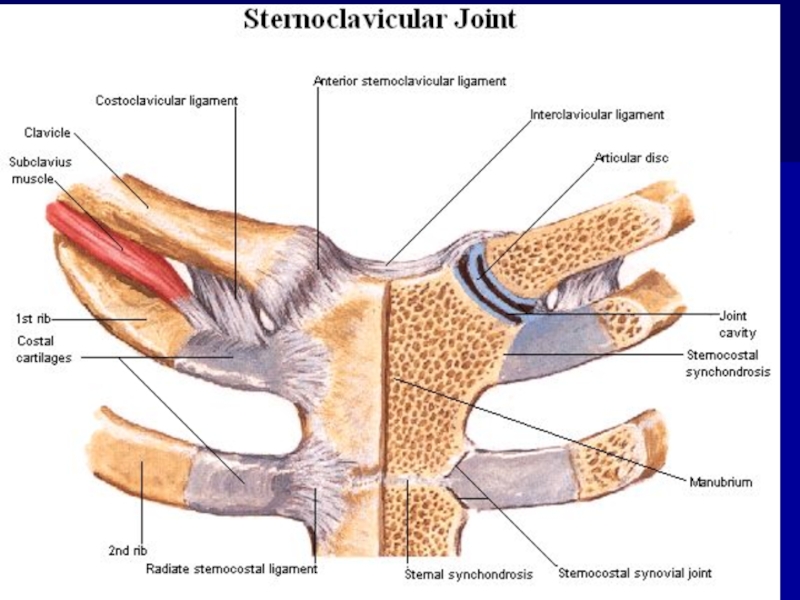
ACCORDING TO THE PROPERTY OF THE CARTILAGINOUS TISSUES : 1—HYALINE— between I rib and sternum.
2—FIBROUS—between vertebral bodies.
These cartilages have no vessels and nerves.

Слайд 15
When ossified, synchondrosis can be transformed
Synostoses or bone articulations (junctura ossea) is contiguous joining of bones by means of bone tissue, for instance, synostoses between three bones of the hip bone in an adult.
.")
Слайд 16SYNOVIAL JOINTS
The synovial articulations
 are discontinuous joints")
Слайд 17THE MOST TYPICAL FEATURES
OF THE JOINTS
Each
articular surfaces, facies articulares;
articular capsule, capsula articularis;
articular cavity, cavitas articularis hermetically sealed, cleft-like cavity; between the articulating bones.
synovial fluid

Слайд 19
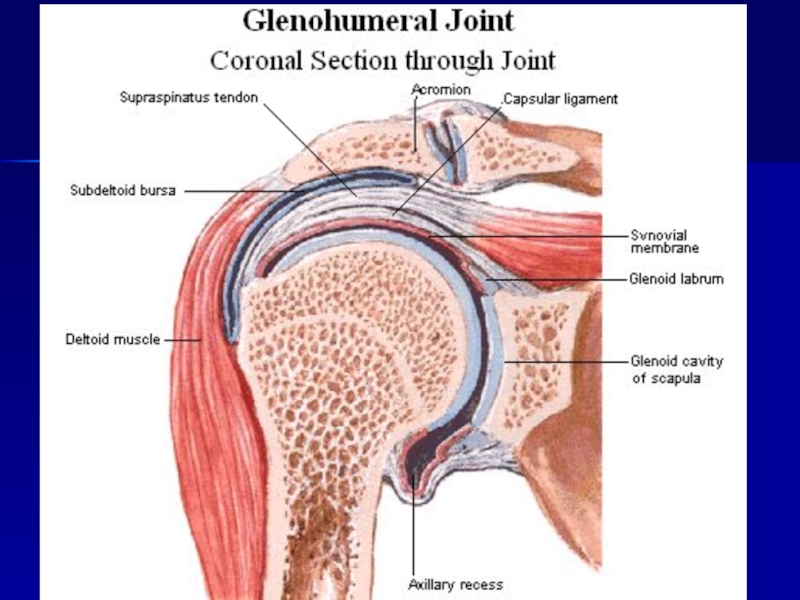
Articular surfaces. The articular
Articular capsule. The capsule of the joint attaches to the edges of articular surfaces or somewhat over them. The articular capsule hermetically seals the articular cavity and consists of two layers - external fibrous layer, membrana fibrosa, and internal synovial layer, membrana synovialis.
The fibrous layer of the capsule has a mechanical function. It consists of bundles of resilient connective tissue fibers, which attach to the bone penetrating it in the form of Sharpie's fibers.
Synovial membrane. This layer of the articular capsule is a thin connective tissue membrane, which is lined on the inside with squamous synovial cells of mesenchymatous origin. Consequently, the synovial membrane can form folds and protrusions.

Слайд 20
Synovial folds and bursae. The synovial membrane is well developed and,
Synovial villi. The synovial layer bears numerous, microscopic, synovial villi, villi synoviales, which significantly increase its surface area, contain capillary networks, and produce the synovial fluid.
Synovial fluid. In the articular cavity there is a small amount of pale, thick, synovial fluid. It is produced by the synovial membrane. The synovial fluid lubricates the articular surfaces and reduces friction between them.
Synovial cavity. Under normal circumstances, the synovial cavity is a thin cleft, bounded by the synovial membrane and the articular surfaces. Between the latter, there is a thin layer of synovial fluid, which separates articulating surfaces. In the pathological processes, the synovial cavity can accumulate large amounts of inflammatory liquid and greatly increases in size.

Слайд 21
Accessory structures of joints
Synovial joints may possess several accessory elements, which facilitate movement to a certain extent:
articular disc, discus articularis, a cartilaginous plate, which completely separates the joint into two regions;
articular meniscus, meniscus articularis, cartilaginous semilunar plate, which partially separates the synovial cavity;
articular lip, labrum articularis, a cartilaginous rim or lip, which deepens the articular socket;
intraarticular ligaments, ligg. intraarticularia, connect bones within the joint; they are covered with the synovial membrane.
Auxiliary strengthening apparatus of joints – ligaments and tendons of muscles. There are extra-articular and intra- articular ligaments, covered by synovial membranes.

Слайд 22Factors, which aid in the stabilization of articular surfaces:
The fibrous
Muscles, which surround the joint and actively hold the bones together due to a constant muscle tone;
Molecular attraction of articular surfaces, lubricated by the synovial fluid.

Слайд 23Congruent and incongruent joints
In those
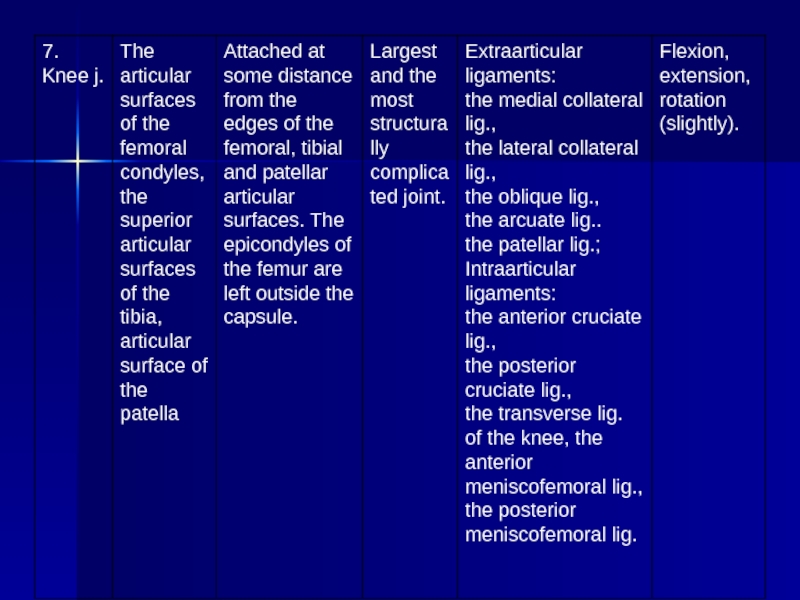
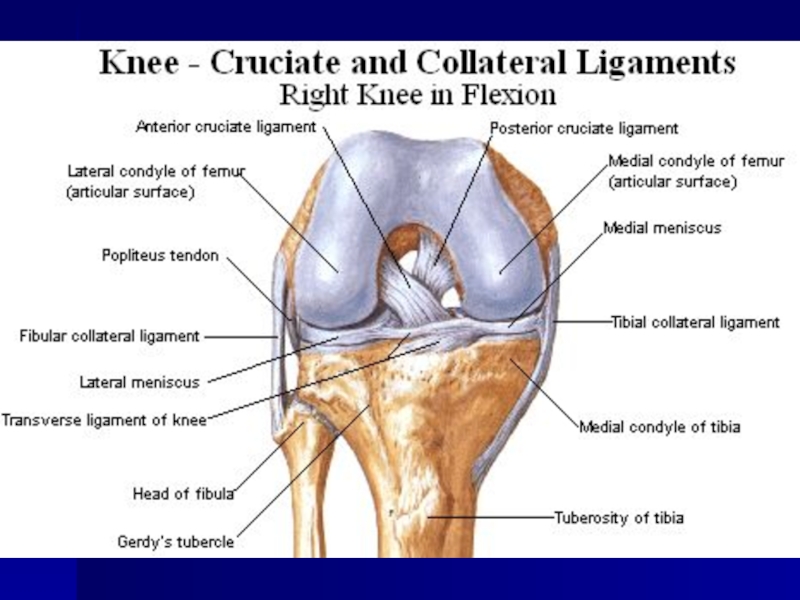
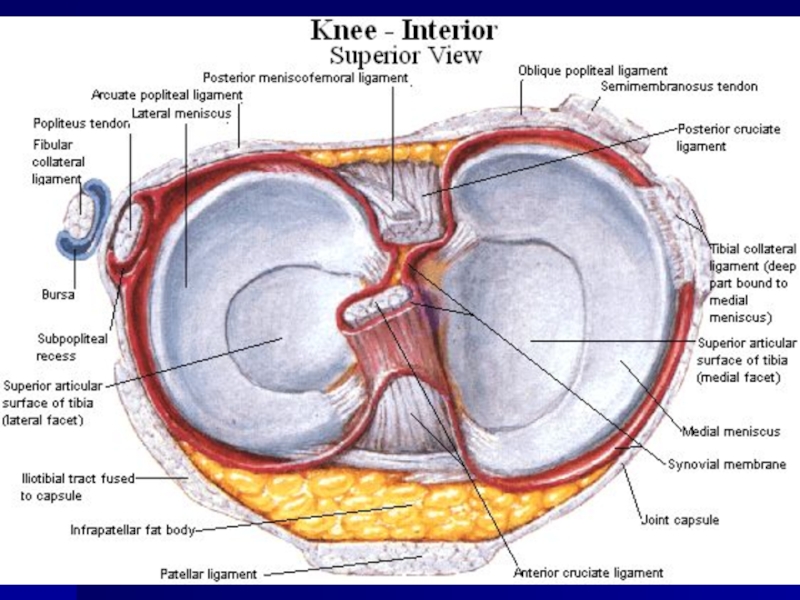
Incongruent joints have a greater degree of freedom in their movements due to the incomplete correspondence of the articulating surfaces. These joints possess accessory structures such as disks, menisci, synovial folds, which fill the irregularities in the articular surfaces and smooth out their incongruence. The knee joint is an example of the incongruent joint.

Слайд 24Movements in the joints
The frontal axis runs through the joint from
The sagittal axis is drawn from front to back. Abduction (abductio) and adduction (adductio) of the shoulder occur around this axis.
The vertical axis runs through the joint and through the entire arm from the top to the bottom. Medial and lateral rotations (rotatio) of the humerus occur around this axis.
Circumduction (circumductio) takes place when the movement passes from one axis to another, as when the hand moves in a circular path. Circular movements are possible in multi-axial and bi-axial joints.

Слайд 25CLASSIFICATION OF JOINTS
Classification of
simple - is composed of only two articulating surfaces;
compound - contains more than two articulating surfaces;
complex joint - if a joint contains articular discs or menisci, which divide it into two parts;
combined joints - two isolated joints, in which movements occur simultaneously.

Слайд 26
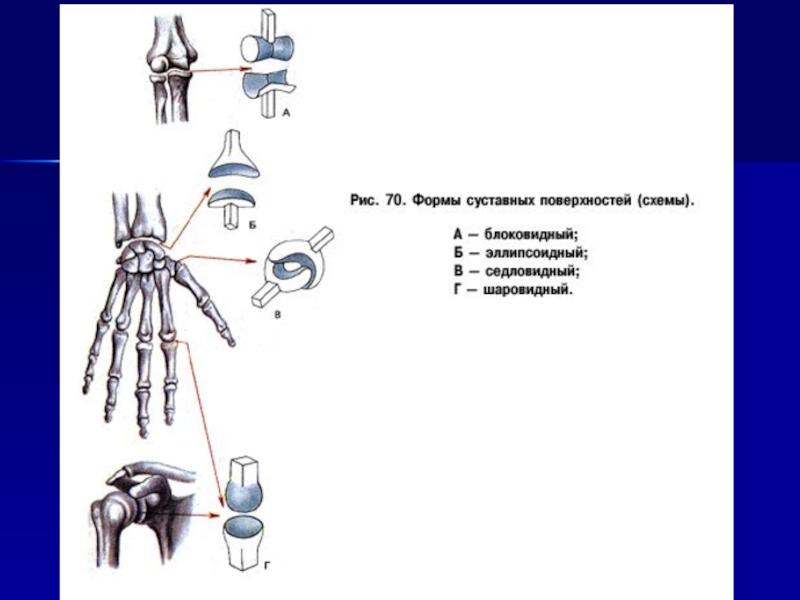
Classification of the joints based on the shape of articulating surfaces:
Bi-axial joints
Multi-axial joints

Слайд 27
Uni-axial joints. In these
hinge joint, ginglymus, contains articulating surfaces, which resemble hinges (for example, interphalangeal joints of the hand and foot);
pivot joint, art. trochoidea (art. cylindrica), a cylindrical joint, formed by the convex and concave articulating surfaces cylindrical in shape (for example, proximal and distal radio-ulnar joints).

Слайд 28
Bi-axial joints. These
ellipsoid joint, art. ellipsoidea, contains elliptical (egg-shaped) articulating surfaces
(for example, radiocarpal joint);
bicondylar joint, art. bicondylaris, consists of a pair of convex, ellipsoid, articulating surfaces, which are rather prominent. Hence, they are known as condyles (for example, knee joint);
saddle joint, art. sellaris, contains two articulating surfaces each of which resembles a saddle
(for example, carpometacarpal joint of the thumb).

Слайд 29
Multi-axial joints include
Even though, in principle, movements in these joints arc possible around multiple axes drawn through the joint, rotation occurs only around three axis:
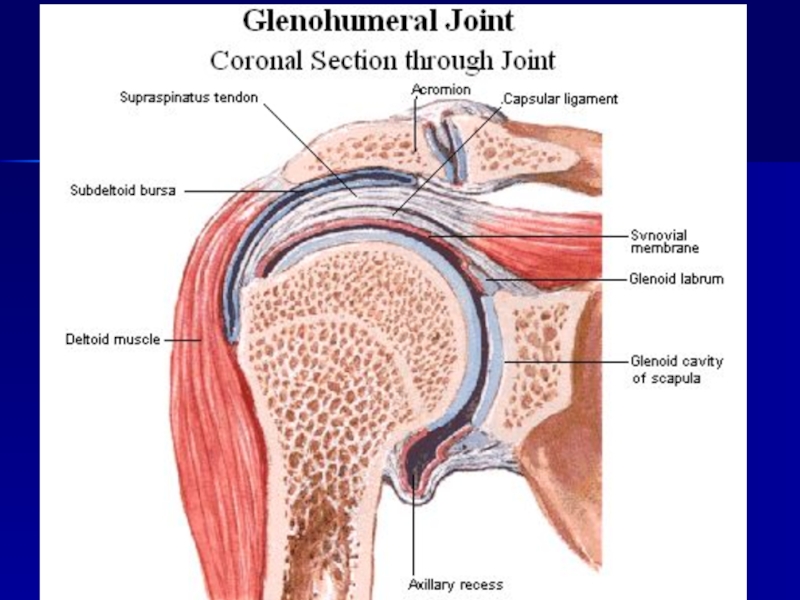
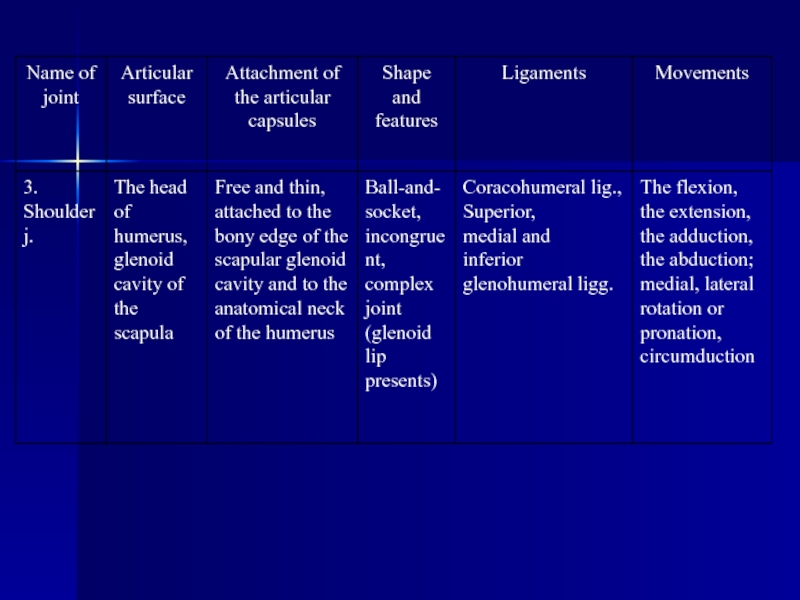
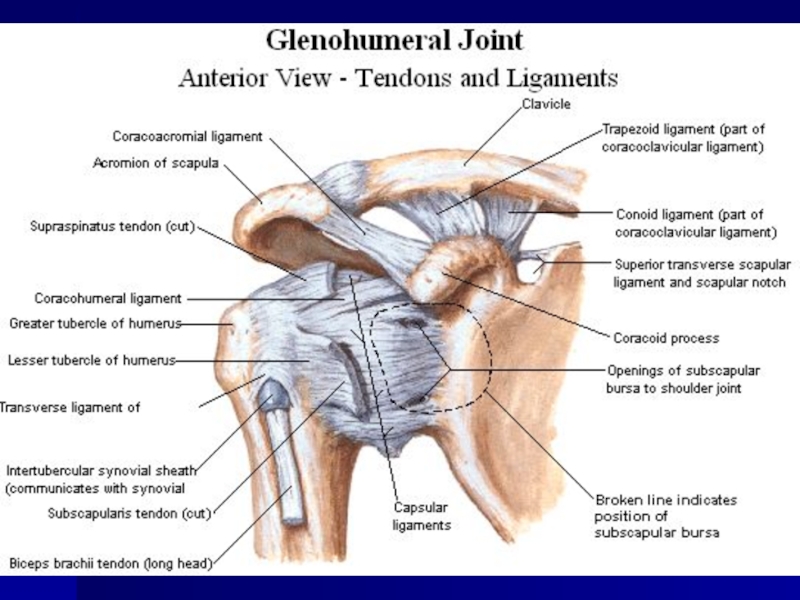
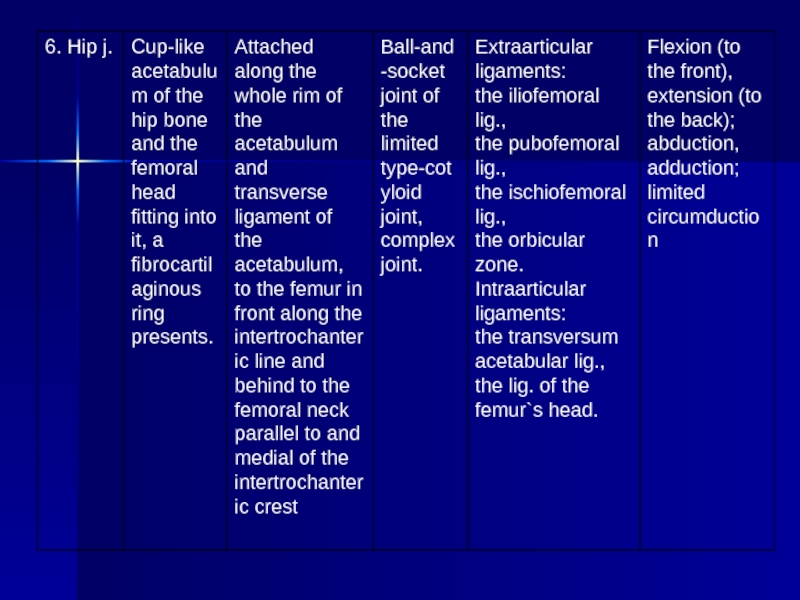
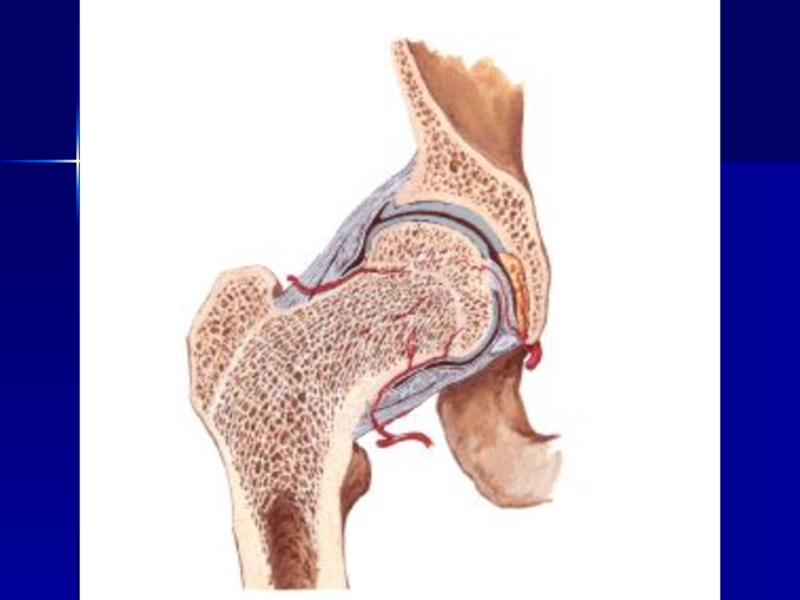
spheroidal joint (ball-and-socket joint), art. spheroidea, consists of a globular head and a corresponding concavity. A typical example is the shoulder joint. Variation of the ball-and-socket joint is the cotyloid joint. Its head resides in a deep articular socket, consequently, it is known as the cup-like joint (art. cotylica);
plane joint, art. plana, contains two flat surfaces, which can be viewed as surfaces of a sphere with a large diameter. Because of the small size difference of both articulating surfaces, only slight translations are possible in plane joints (for example, sacroiliac joint).

Слайд 31Clinical applications
Pathological process can

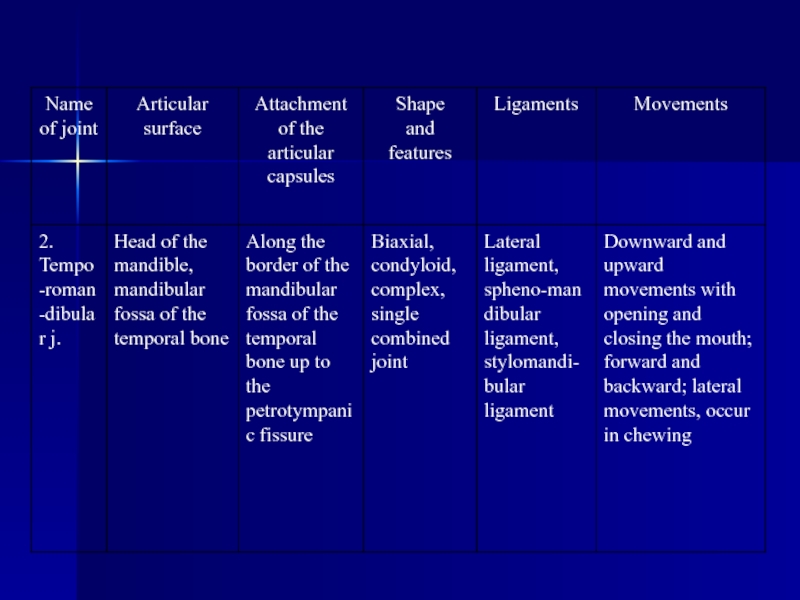
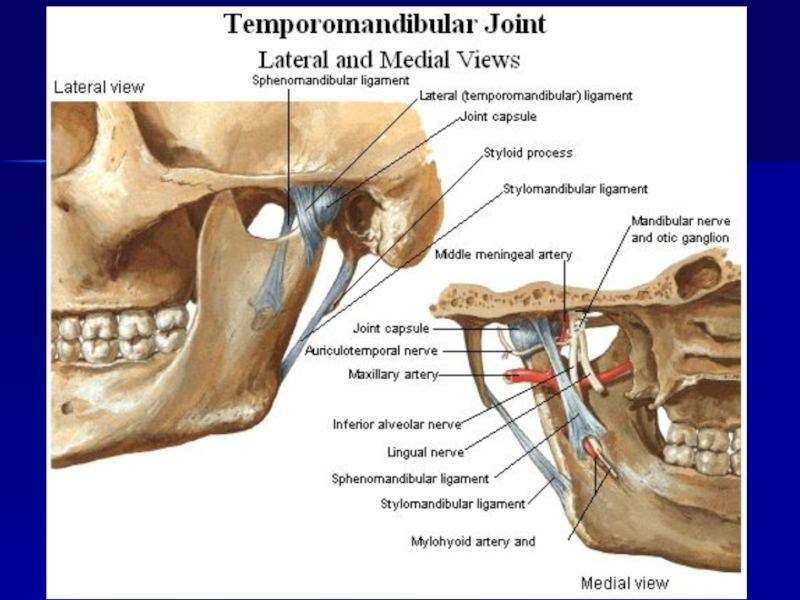
Слайд 53THE TEMPOROMANDIBULAR JOINT
The temporomandibular joint, articulatio temporomandibularis, is
It belongs to the group of the bicondylar, combined joints.
The articular surfaces are incongruent. Therefore, inside the joint there is the articular disk, discus articularis, which fuses with the fibrous capsule and divides the articular cavity of the joint into two isolated levels - the upper and the lower (complex joint).
Fibrous capsule. In the region of the temporal bone, the capsule is attached to the margins of the mandibular fossa, fossa mandibularis, covers in the front the articular tubercle, tuberculum articulare, and in the back reaches the petrotympanic fissure. On the mandible, the capsule attaches to the edge of the articular surface of the head in the front (above the pterygoid fossa), while in the back it inserts into the neck of the mandible.

Слайд 54
Ligaments.
The capsule is reinforced by the lateral ligament, lig. laterale,
1) lig. stylomandibular, which runs from the styloid process of the temporal bone to the posterior angle of the mandible;
2) lig. sphenomandibulare, which extends from the spine of the sphenoid towards the lingula of the mandible.
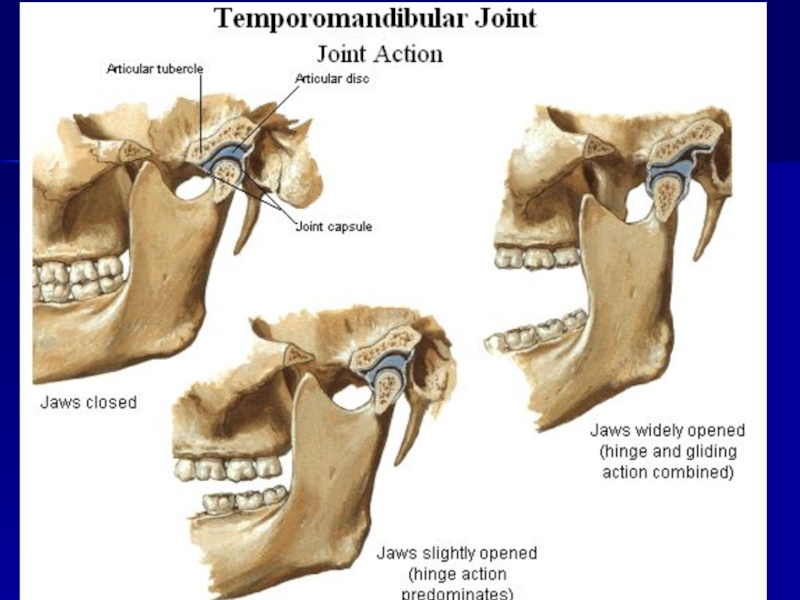
Movements. The temporomandibular joint permits the following movements:
1) elevation and depression of themandible occurs around the frontal axis in the lower level of the joint. When the mandible is exceedingly depressed, the articular disk with the head of the mandible may be displaced onto the articular tubercle;
2) protrusion of the mandible occurs in the upper level of the joint in such a way that the head together with the articular disk are drawn onto the articular tubercle;
3) lateral movements of the mandible occur such that on one side the head remains in the fossa, whereas on the opposite side it: is drawn onto the articular tubercle together with the articular disc.

Слайд 55MASTICATORY MUSCLES
The masticatory muscles are derived from the common mesenchymatous primordium
THE SUPERFICIAL MASTICATORY MUSCLES
Masseter, m. masseter.
Origin: zygomatic arch.
Insertion: masseteric tuberosity and angle of the mandible. It consists of two parts — superficial (pars superficialis) and deep (pars profunda).
Action. Elevates the mandible; the superficial part protracts the mandible.
Temporalis, m. temporalis.
Origin: temporal and parietal bones, temporal fascia.
Insertion: coronoid process of the mandible. The muscle fills the temporal fossa. It is flat and fan-shaped. The anterior fibers of the temporalis are directed vertically, middle fibers — obliquely, and posterior fibers — almost horizontally. The fibers of the muscle converge below forming a thick tendon, which runs underneath the zygomatic arch and inserts into the coronoid process.
Action. Elevates and retracts the mandible.

Слайд 56THE DEEP MASTICATORY MUSCLES
Medial pterygoid, m. pterygoideus medialis.
Origin: pterygoid fossa of
Insertion: pterygoid tuberosity of the mandible.
Action. Elevates and pulls the mandible to the side. When the muscle contracts on both sides, it protracts the mandible.
Lateral pterygoid, m. pterygoideus lateralis.
Origin: arises by two heads: from the infratemporal crest of the sphenoid bone (upper head) and lateral plate of the pterygoid process (lower head).
Insertion: pterygoid fossa of the neck of the mandible and capsule of the temporomandibular joint.
The muscle is triangular in shape. Its fibers are directed backward and laterally. It lies deep in the infratemporal fossa covered by the zygomatic arch and the ramus of the mandible as well as by the temporal muscle.
Action. In unilateral contraction, the muscle moves the mandible to the opposite side; when the lateral pterygoid muscles of the two sides act together they protrude the mandible.
Nerve supply of the masticatory muscles. All masticatory muscles arc supplied by the third branch of the trigeminal nerve.

Слайд 57Muscles of the neck
Is divided into three groups: - Superficial
- deep
Superficial Muscles of the neck
1. The platysma is subcutaneous muscle, which attached from the 2 rib to the mandible.
Action: - pulling the skin of the neck;
- depress the angle of the mouth.
2. The sternocleidomastoid muscle lies under the platysma.
Attached: - the hilt of sternum
- the sternal and of the clavicle
- the mastoid process
- the superior nuchae line.
Action: - hold the head in a vertical position

Слайд 58Middle muscles of the neck
Is divided into 2 groups: - above
Muscles located above the hyoid bone
The mylohyoid muscle is flat, connected to the mylohyoid muscle.
2. The digastric muscle consists of two bellies. Anterior arises from the digastrics fossa, posterior – the mastoid process.
3. The stylohyoid muscle – the styloid process of temporal bone.
4. The geniohyoid muscle – lies above the mylohoid muscle on the mental spine of mandible.

Слайд 59Muscles located below the hyoid bone
1. The sternohyoid muscle attached the
Action: - pulls the hyoid bone downwards.
2. The sternothyroid muscle: - lies under the sternohyoid muscle, lowers the larynx.
3. The thyrohyoid muscle is continuated of the sternothyroid muscle, pulls the larynx upwards.
4. The omohyoid muscle – consists of two bellies, inferior and superior. Inferior arises of the subscapular notch and connected with superior belly.
Action: pulls the hyoid bone downwards.

Слайд 60The Deep muscles of the neck
Is divided into three groups: -
- prevertebral
- suboccipital
The Deep lateral muscles of the neck
1. The anterior scalene muscle
2. The medius scalene muscle
3. The posterior scalene muscle
They attached the transverse processes of the cervical vertebrae.
Action: raises the upper ribs, inspiration muscles.
The Deep prevertebral muscles of the neck
1. The long muscle of the neck
2. The long muscle of the head
Action: flex the head forward and laterally
The Deep suboccipital muscles of the neck
1, 2. The anterior and lateral straight muscles of the head – flex the head forward, spine – laterally.
3, 4. The obliquus capitis superior and inferior muscles
5, 6. The greater and lesser straight muscles
Action: rotate the head and pull it backwards.